The Times They Are A Changin': the "No Zone" Approach to Management of Penetrating Neck Trauma
Clinical Case: You're working a busy evening shift when a middle aged woman is brought in by EMS from the scene of a car accident. She has a deep laceration to her anterior neck near the level of the
cricoid cartilage from a glass shard. She is neurologically intact, talking with a normal voice and is in no
respiratory distress. However, there is a continuous and brisk oozing of
blood from the wound.
Clinical Question: What imaging is indicated in hemodynamically stable, neurologically intact patients with penetrating neck injuries? What should the typical disposition be?
Literature Review:
Any neck wound that extends deep to the platysma is
considered a penetrating neck wound, and it is estimated that they
represent 5-10% of all trauma patients who arrive to the emergency
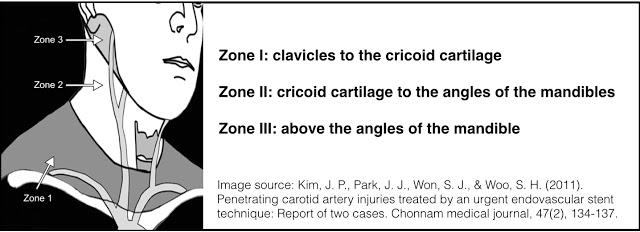
department. Two common ways of anatomically dividing
the neck include using the sternocleidomastoid to divide the neck into
anterior and posterior triangles, or dividing the neck into three zones [1]:
 In the event of penetrating injury to the neck, airway compromise should be immediately assessed, with early intubation for airway protection if there is any concern for expanding neck hematoma or concerns for airway injury. An attempt can be made to orotracheally intubate (bougies have been suggested as excellent initial adjuncts [2]), but plans should be made to move to early cricothyroidotomy if the airway is unable to be secured from above. After
securing the airway and establishing hemodynamic stability, the neck
wound should be carefully inspected. Injuries that breach the platysma may have caused significant underlying injury, and it is best to
avoid probing these wounds at the bedside, as
this could disrupt hemostasis. Aside from risk of vascular disruption, patients with
penetrating neck injuries warrant consideration of tracheal and
esophageal compromise. Signs of tracheal injury include air bubbling at
the wound, hemoptysis, subcutaneous emphysema, and stridor. Esophageal injuries can be
initially be asymptomatic, and a missed injury can lead to neck space
infection and mediastinitis [3].
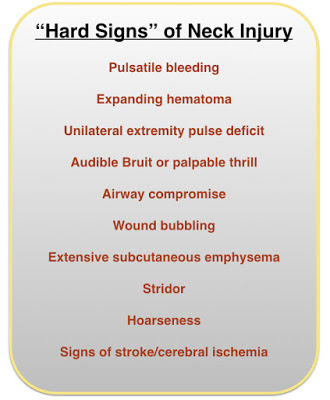
Emergent surgical consultation is
warranted, as patients with hemodynamic instability and/or "hard signs" of vascular or aerodigestive tract injury should go for emergent neck exploration [3].
In the event of penetrating injury to the neck, airway compromise should be immediately assessed, with early intubation for airway protection if there is any concern for expanding neck hematoma or concerns for airway injury. An attempt can be made to orotracheally intubate (bougies have been suggested as excellent initial adjuncts [2]), but plans should be made to move to early cricothyroidotomy if the airway is unable to be secured from above. After
securing the airway and establishing hemodynamic stability, the neck
wound should be carefully inspected. Injuries that breach the platysma may have caused significant underlying injury, and it is best to
avoid probing these wounds at the bedside, as
this could disrupt hemostasis. Aside from risk of vascular disruption, patients with
penetrating neck injuries warrant consideration of tracheal and
esophageal compromise. Signs of tracheal injury include air bubbling at
the wound, hemoptysis, subcutaneous emphysema, and stridor. Esophageal injuries can be
initially be asymptomatic, and a missed injury can lead to neck space
infection and mediastinitis [3].
Emergent surgical consultation is
warranted, as patients with hemodynamic instability and/or "hard signs" of vascular or aerodigestive tract injury should go for emergent neck exploration [3].Classically, management of hemodynamically stable patients with penetrating neck injuries was based on an anatomic "zone-based" approach mentioned above, with zone II injuries often going directly to surgical exploration and zone I and III injuries undergoing angiography, bronchoscopy, and esophagoscopy. This approach was developed in the 1970’s, but it had several problems [4]. First, there may be poor correlation between the location of the neck wound and internal organ involvement, as there may be traversing of zones internally. Secondarily, the adoption of a mandatory-exploration policy lead to a high negative exploration rate (53% - 56%)[4,5].
With the rapid improvement and dissemination of the use of CT over the past few decades, a “No Zone” management approach based on careful physical exam with CT angiography has been shown in surgical literature to decrease resource utilization and unnecessary surgical exploration, making the rigid zone approach less relevant [3]. Several studies have examined the sensitivity and specificity of CT angiography in stable patients with penetrating neck injury. A study by Inaba et. al. prospectively evaluated an algorithm in which patients with "soft signs" of injury (venous oozing, non-expanding hematoma, minor hemoptysis, dysphonia, dysphagia, or small amount of subcutaneous emphysema) underwent an initial evaluation with CT-angiography and asymptomatic patients were observed [6]. Over a 31-month period, 453 patients with penetrating neck trauma were prospectively evaluated in their study. 186 of these patients had "soft signs" of clinical injury, and underwent CT angiography as their initial method of evaluation. 38.2% of these patients had an injury to zone II of the neck. Using an aggregate gold standard of the final diagnosis at discharge which included operative exploration, catheter-based angiography, bronchoscopy, esophagogram and esophagoscopy results and clinical follow-up (duration not specified), the sensitivity and specificity of CT Angiography for vascular or aerodigestive injury was 100% and 97.5 % respectively. There were two patients who had false-positive findings of vascular injury (irregularities in the ICA) that were not present on follow-up with surgical exploration and/or angiography, and three patients had air tracking suspicious for aerodigestive tract injury that was not confirmed on follow-up imaging and endoscopic studies.
As mentioned above, the "No Zone" approach combining clinical exam with imaging evaluation has the potential to decrease unnecessary neck exploration. A study by Osborn et. al. examined the rate of negative neck explorations in patients who were taken to the OR who did not have hard signs of injury. They compared the rate of negative neck explorations amongst those patients who had a CT-A as part of their initial evaluation and those who did not, and found that CT angiography significantly reduced the negative neck exploration rate [7]:
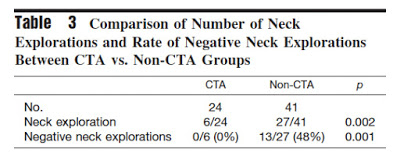 |
| Source: Osborn et al. (2008) |
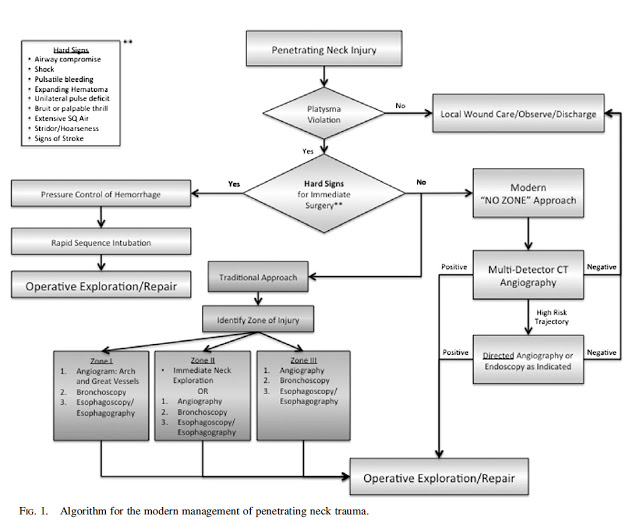 |
| Image Source: Reference 3 |
Take Home Points: Patients with penetrating neck trauma who are hemodynamically unstable or display hard signs of vascular or aerodigestive should receive immediate surgical consultation with consideration for operative or invasive management. As the traditional, anatomic approach to management of penetrating neck
trauma is associated with a high rate of negative neck exploration, patients with soft signs of injury should be initially evaluated with CT angiography which has a high sensitivity for clinically-significant injury.
Submitted by Philip Chan, PGY-3
Edited by Maia Dorsett (@maiadorsett), PGY-4
Faculty reviewed by jason wagner (@TheTechDoc)
Submitted by Philip Chan, PGY-3
Edited by Maia Dorsett (@maiadorsett), PGY-4
Faculty reviewed by jason wagner (@TheTechDoc)
References
[1] Tintinalli’s Emergency Medicine, 7e. Ch 257.
[1] Tintinalli’s Emergency Medicine, 7e. Ch 257.
[2] Daniel, Y., de Regloix, S., & Kaiser, E. (2014). Use of a Gum Elastic Bougie in a Penetrating Neck Trauma. Prehospital and disaster medicine, 29(02), 212-213.
[3] Shiroff, A. M., Gale, S. C., Martin, N. D., Marchalik, D., Petrov, D., Ahmed, H. M., ... & Gracias, V. H. (2013). Penetrating neck trauma: a review of management strategies and discussion of the ‘No Zone’approach. The American Surgeon, 79(1), 23-29.
[4] Prichayudh, S., Choadrachata-anun, J., Sriussadaporn, S., Pak-art, R., Sriussadaporn, S., Kritayakirana, K., & Samorn, P. (2015). Selective management of penetrating neck injuries using “no zone” approach. Injury.
[5] Varghese, A. (2013). Penetrating neck injury: a case report and review of management. Indian Journal of Surgery, 75(1), 43-46.
[6] Inaba, K., Branco, B. C., Menaker, J., Scalea, T. M., Crane, S., DuBose, J. J., ... & Demetriades, D. (2012). Evaluation of multidetector computed tomography for penetrating neck injury: a prospective multicenter study. Journal of Trauma and Acute Care Surgery, 72(3), 576-584.
[3] Shiroff, A. M., Gale, S. C., Martin, N. D., Marchalik, D., Petrov, D., Ahmed, H. M., ... & Gracias, V. H. (2013). Penetrating neck trauma: a review of management strategies and discussion of the ‘No Zone’approach. The American Surgeon, 79(1), 23-29.
[4] Prichayudh, S., Choadrachata-anun, J., Sriussadaporn, S., Pak-art, R., Sriussadaporn, S., Kritayakirana, K., & Samorn, P. (2015). Selective management of penetrating neck injuries using “no zone” approach. Injury.
[5] Varghese, A. (2013). Penetrating neck injury: a case report and review of management. Indian Journal of Surgery, 75(1), 43-46.
[6] Inaba, K., Branco, B. C., Menaker, J., Scalea, T. M., Crane, S., DuBose, J. J., ... & Demetriades, D. (2012). Evaluation of multidetector computed tomography for penetrating neck injury: a prospective multicenter study. Journal of Trauma and Acute Care Surgery, 72(3), 576-584.
[7] Osborn, T. M., Bell, R.
B., Qaisi, W., & Long, W. B. (2008). Computed tomographic
angiography as an aid to clinical decision making in the selective
management of penetrating injuries to the neck: a reduction in the need
for operative exploration. Journal of Trauma and Acute Care Surgery, 64(6), 1466-1471.