A 25 y.o. woman with a hx of headaches comes to the ED because she was told her MRI was abnormal.
She had gone to an outpatient MRI facility.
what is wrong? What needs to be done?
Our patient had empty sella syndrome(ESS). 12% of individuals who have advanced imaging will have this finding. Where the pituitary sits in the sella, there is herniation of the subarachnoid space with compression of the pituitary gland. The sella is filled with CSF.
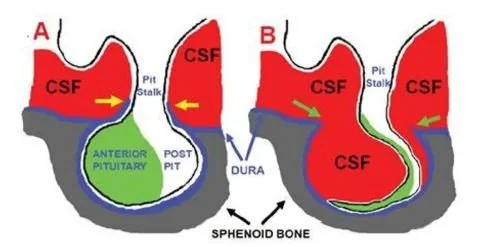
with compression of the pituitary necrosis occurs.
CLINICAL PRESENTATION
Our patient presented with headaches. Headaches, fatigue, irregular menstrual periods erectile dysfunction and galactorrhea can be signs of empty sella syndrome because of increased intracranial pressure or pituitary dysfunction.
Empty sella syndrome which is incidentally discovered often has no clinical consequences, but recent longitudinal studies estimate that 15-20% of patients will have hypoadrenalism, hypothyroidism and hypogonadism even without symptoms. It is recommended that all patients receive hormone testing.
Traditionally, empty sella syndrome is divided into two forms.
Primary Empty Sella Syndrome
Primary empty sella syndrome occurs when there is a congenital defect in the diaphragma sellae allowing CSF to flow into the sella which compresses the pituitary. Often occurs in obese middle aged women with hypertension. It is commonly diagnosed in women with pseudotumor cerebri.
Secondary Empty Sella Syndrome
Secondary empty sella syndrome can occur after a head injury because of vascular injury to the pituitary causing it to shrink. This also occurs with tumors which apply pressure to the pituitary and cause the gland to necrose. Craniopharyngiomas an example of this. Infections, infiltrative diseases like histiocytosis , and autoimmune inflammation caused by checkpoint inhibitors can all cause swelling of the pituitary and eventual shrinkage due to tissue death.
WHAT SHOULD BE DONE IN THE ED?
In addition to referring the patient to an endocrinologist for an evaluation of pituitary function you could:
1. Look for papilledema and consider pseudotumor.
2. Draw a prolactin and TSH/ T4. Prolactin is elevated in many pituitary tumors because compression of the pituitary stalk blocks dopamine going to the anterior pituitary from the hypothalamus. With the body’s prolactin inhibiting factor blocked there is unchecked release of prolactin. This is especially useful if there is a delay in seeing an endocrinologist.
3. Ask about menses in women and libido in men since gonadotrophins are often the first hormones to be affected.
4. Optionally, if it is near 8 am, draw a cortisol. If the patient works nights forget that since AM cortisol is not helpful.
TREATMENT
1. The treatment depends on the cause. Pseudotumor is treated with Diamox or in extreme cases with optic nerve sheath fenestration, shunts or venous sinus stenting. Craniopharyngiomas are treated with surgery and radiation followed by replacement hormones.
Our patient was evaluated for hormone dysfunction and none was found. She had a normal pressure on her LP and no evidence of immune dysfunction. She is being treated symptomatically for headaches and being followed by an endocrinologist.
chronic fatigue alters cortisol
FUN FACT
If the patient works nights AM cortisol is not helpful. This is because circadian rhythms are either altered or not present in shift workers, those who travel across time zones, or blind individuals. Chronic fatigue also alters cortisol. The body can overproduce cortisol at night as a result making it difficult to sleep.
Ahamed M A A, Shetty S, Hegde S, et al. (September 08, 2022) The Emptiness Within: A Case of Empty Sella Syndrome. Cureus 14(9): e28941. doi:10.7759/cureus.28941
Chiloiro S, Giampietro A, Bianchi A, Tartaglione T, Capobianco A, Anile C, De Marinis L: Diagnosis of endocrine disease: primary empty sella: a comprehensive review. Eur J Endocrinol. 2017, 177:R275-R285
Carosi G, Brunetti A, Mangone A, et al. a multicenter cohort sturdy in patients with primary empty sell: hormonal and neuroradiological features ove a long follow -up. Front Endocrinol 2022. Jun 23;13:925378,
Lundholm M, Yogi=Marren D. A comprehensive review of empty sella and empty sella syndrome. AACE Endocrine Practice. May 2024 Vol 30(4).:397-502.
Brum M, Senger M, Schnorr C. Effect of night-shift work on corticol circadian rhythm and melatonin levels. Sleep Sci. 2022 Apr-June;15(2):143=148,