A 50 y.o. woman comes to the ED with sore throat, cough and fever
Below are her CXR and a photo of the oropharynx. Hint: the lateral xray holds the key.


do you notice a peripheral wedge shaped opacity?

What systemic disease could present with these findings?
Our patient had a wedge-shaped defect seen best on the lateral CXR. This “ Hampton’s hump” is suggestive of a pulmonary embolus since it touches the pleura. If this is combined with the image of oral ulcers, it suggests a more systemic disease. Our patient had lupus with a circulating lupus anticoagulant causing the pulmonary embolus.
Systemic lupus erythematosus (SLE) is an autoimmune disease in which individuals develop antibodies to their own DNA. It occurs 90% of the time in women. Interestingly it has been linked to incomplete inactivation of the second X chromosome in women.
While recent research is being done on genetic defects predisposing to lupus, the disease itself is ancient. It was first described in the 10th century, but named in 13th century by Rogerius. It was named “lupus” because often multiple skin lesions occur which were thought to resemble wolf bites. Osler was the first to describe multiple systemic lesions with lupus including kidney, heart and brain.

SYSTEMIC INVOLVEMENT CAN INCLUDE THE FOLLOWING:
Mucocutaneous lesions-In addition to the classic malar rash, vasculitic ulcers can appear on any part of the body.. Painless, shallow oral ulcers, most often occur on the hard and soft palate. Oral ulcers occur at onset in 11% of patients, while at any time are present in 30% of patients.
Hematologic manifestations-Antiphospholipid syndromes- lupus anticoagulant, anticardiolipin antibodies and anti beta2-glycoprotein-1 antibodies can produce thrombosis and pulmonary emboli. Clots also lead to miscarriages. Anemia and thrombocytopenia are common.
Musculoskeletal involvement-90% of individuals with SLE have joint involvement. Osteonecrosis is a complication.
Renal involvement- Vasculitis of small sized vessels can result in nephritis with hypertension and edema or nephotic syndrome with proteinuria.
Neuropsychiatric involvement- Lupus can present with cerebritis, stroke or psychosis.
Cardiovascular involvement- asymptomatic pericarditis is the most frequent manifestation of lupus involving 40% of patients. Accelerated coronary disease occurs.
Pulmonary involvement- 45-60% present with pleuritis or pleural effusions.
GI involvement- serositis may produce abdominal pain. Mesenteric vasculitis and peritonitis are serious complications.
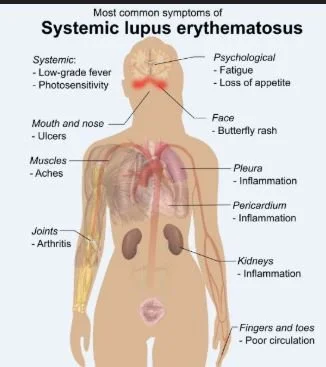
lupus is a systemic disease
• Anti-dsDNA antibodies are specific for the disease (95-98%). ANA and anti-Sm antibodies are not specific for SLE but suggest an autoimmune process. Our patient was positive for anti-dsDNA antibodies.
She was treated with warfarin because direct oral anticoagulants are not recommended with a circulating lupus anticoagulant. She was treated for her lupus with plaquenil and eye exams were scheduled.
FUN FACT
One of the findings on a non contrast CT that suggests a pulmonary infarct is the “bubble sign” It is a highly specific marker for PE. The necrotic lung shows areas of gas as in the image below.

the bubble sign of a pulmonary infarct
Leone P, Prete M, Malerba E, et al. Lupus vasculitis: an overview Biomedicines. 2021 Nov 5;911):1626.
MKSAP 19 Rheumatology pp.42-48
Payus A, Raiah R, Febriany D. Pulmonary embolism masquerading as severe pneumonia: a case report.Open Access Maced J Med Sci. 2019 Feb 10;7(3):396-399.
Kowal D. Radiologist HQ.com Case of the Week #9
Justinussen T, Gram J, Bor M. Antiphospholipid antibodies in pulmonary embolism treated with direct oral anticoagulants :prevalence data from unselected consecutive patients. Res Pract Thromb Haemost. 2023 Jan 18;7(1): 100050.