Consultant Teachings No. 3: Evaluation of Tendinous Hand Injuries for the Emergency Provider
Clinical Case: You are working in a community emergency department one evening when a woman presents with a laceration across the fingerpad of her right thumb that she sustained after falling onto a piece of glass. The laceration itself is pretty small - about a centimeter across - and has minimal bleeding. The X-ray ordered by the triage nurse is negative for retained foreign body. Before you just sew this up and send the patient on her way, you appropriately decide to do a thorough hand exam, including for tendonous injury. The patient keeps saying that its hard to bend her finger because it hurts...
Consultant Teaching: Tendon Injuries to the hand are often complex entities that are subject to ongoing research regarding optimal procedures for management and rehabilitation. The flexor and extensor tendon anatomy is quite complex. Both are divided into numerous “zones” created to help clarify the optimal treatment, which can vary markedly depending on injury location. Missed tendon injuries increase morbidity by complicating later management and are therefore a leading cause of malpractice claims in the world of Emergency Medicine. The most important and fundamental aspect of evaluation in these patients is a detailed hand exam. Outlined below is a guide for the evaluation and management of any patient presenting to the ED with a suspected hand injury.
Flexor Tendon Injuries
The first step is to obtain a detailed history of the mechanism of injury. Was the injury caused by a rusty farm knife or a sharp chard of glass? What was the position of the patient’s hand when the injury occurred? This is a frequently missed point to mention. You can imagine that, if the patient was lacerated with flexed fingers while gripping a knife, the location of the tendon injury itself may be in a very different location than the skin laceration when evaluating the hand in a more extended posture. Just because you can no longer see the damaged tendon in the wound doesn’t mean it’s not there.
Step 1: Observation
Evaluate the location and depth of the laceration. Look at the resting posture of the hand and the
 patient’s digital cascade. When in doubt, you can usually find clues by looking at the resting finger position of the uninjured hand. Your clinical suspicion should be raised if a particular finger rests in a more extended position relative to the others.
patient’s digital cascade. When in doubt, you can usually find clues by looking at the resting finger position of the uninjured hand. Your clinical suspicion should be raised if a particular finger rests in a more extended position relative to the others.
Step 2: Passive Range of motion
These hand injuries can be really painful. A good place to start is assessment of passive motion with a maneuver that elicits the tenodesis effect. Try it on yourself - With a relaxed hand, when you passive flex your wrist, your MCP/PIP/DIP joints will extend. Similarly, wrist extension will cause passive flexion of those digits. If you passively extend the patient’s wrist and there is persistent extension of the DIP or PIP joints, you may have a flexor tendon injury in that digit.
Step 3: A detailed (ie purposeful) neurovascular exam
Flexor tendon injuries are frequently associated with neurovascular injury because of the palmar
 location of these structures. The best way to assess nerve function is with a two-point discrimination exam. This can easily be performed with a paper clip. Remember that each finger has proper digital nerves on its palmar aspect on both the radial and ulnar sides: test them both. *Tip 1* If you get abnormal results that don’t make sense given the injury, test the other hand! Your patient who forgot to mention his terrible neuropathy will appreciate this. *Tip 2* Under NO circumstances should a digital block be performed if you are planning to consult the hand service on call. If analgesia is an issue, let the hand service know and proceed with necessary oral/IV medications until your consulting service is able to evaluate the patient’s neurovascular status. This is not only important for our documentation, but is critical for possible surgical planning.
location of these structures. The best way to assess nerve function is with a two-point discrimination exam. This can easily be performed with a paper clip. Remember that each finger has proper digital nerves on its palmar aspect on both the radial and ulnar sides: test them both. *Tip 1* If you get abnormal results that don’t make sense given the injury, test the other hand! Your patient who forgot to mention his terrible neuropathy will appreciate this. *Tip 2* Under NO circumstances should a digital block be performed if you are planning to consult the hand service on call. If analgesia is an issue, let the hand service know and proceed with necessary oral/IV medications until your consulting service is able to evaluate the patient’s neurovascular status. This is not only important for our documentation, but is critical for possible surgical planning.
There are multiple ways to assess the vascular status. Assessment of cap refill, a digital Allen’s test (same concept as the wrist, but with compression of the radial and ulnar palmar arteries of each finger) and pulse oximetry can all help establish whether or not a concomitant vascular injury is present.
Step 4: Flexor Tendon Exam
 A quick anatomy review is necessary here because, in the hand, form truly follows function. The flexor digitorum profundus (FDP) and superficialis (FDS) tendons are both extrinsic hand muscles that power finger flexion. The FDP lies deep to FDS and then attaches distally to the distal phalanx of the 2nd-5th digits. The FDS attaches at the base of the intermediate phalanx of these digits. Why is that important to know for your physical exam? Since these muscles share a common belly and are intimately associated with one another, you must carefully isolate the desired tendon on each digit. Asking a patient to “wiggle their fingers” is an easy way to improperly assess hand function and miss isolated tendon injuries. To test the FDS: all adjacent digits must be held with all joints in extension while the patient flexes the finger at the PIP joint. To test the FDP: hold the middle phalanx in extension while asking the patient to flex just their distal phalanx. Another reason not to digital block these patients is that pain with these movements may clue the examiner into a possible partial tear or laceration.
A quick anatomy review is necessary here because, in the hand, form truly follows function. The flexor digitorum profundus (FDP) and superficialis (FDS) tendons are both extrinsic hand muscles that power finger flexion. The FDP lies deep to FDS and then attaches distally to the distal phalanx of the 2nd-5th digits. The FDS attaches at the base of the intermediate phalanx of these digits. Why is that important to know for your physical exam? Since these muscles share a common belly and are intimately associated with one another, you must carefully isolate the desired tendon on each digit. Asking a patient to “wiggle their fingers” is an easy way to improperly assess hand function and miss isolated tendon injuries. To test the FDS: all adjacent digits must be held with all joints in extension while the patient flexes the finger at the PIP joint. To test the FDP: hold the middle phalanx in extension while asking the patient to flex just their distal phalanx. Another reason not to digital block these patients is that pain with these movements may clue the examiner into a possible partial tear or laceration.
For completeness, it is also important to document motor testing for all muscles with separate nerve innervations, regardless of its proximity to the wound in question.
Extensor Tendon Injuries
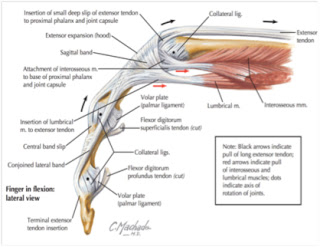
Like the flexor tendons, these also can be diagnostic challenges due to the complex anatomy of the extensor mechanism. This region is comprised of extrinsic muscles that power digit extension, like the extensor digitorum communis (EDC) and an extensor aponeurosis with multiple connecting bands and ligaments. Again, a detailed history will provide valuable insight and context for your exam. Is it a result of a fight-bite injury? A crushing mechanism?
The general principles of the physical exam addressed above regarding observation, passive range of motion and a detailed neurovascular exam still apply. As diagrammed in the image above, for the dorsal hand, it is especially important to assess both the radial and ulnar nerves.
With regard to hand posture, take note if there is a resting flexed position of the digit, a mallet finger, or boutonniere deformity. This should heighten your suspicion for a tendon injury.
Assessment of the Extensor Tendon
A few important considerations are noteworthy here. First, do not be fooled by the action of the lumbricals! Remember, these muscles provide extension of the PIP and DIP joints via the lateral bands. Have the patient lay their hand flat on a table (extends the MCP joint and helps remove the influence of lumbricals) and extend at the MCP joint against resistance. Extension along an affected digit may still be possible even after complete laceration, due to the multiple contributions to the extensor mechanism. Look closely for a lack of hyperextension or differential extension in the affected finger that may be a sign an extensor tendon injury has occurred. The junctura tendinae are intertendinous fascial connections located around the MCP joint that attach tendons of the EDC and help coordinate their movements. This anatomic structure is important to keep in mind because the junctura may allow for some extension of an injured digit if the tendon injury is proximal to them.
Lastly, if you are concerned about an injury to the “central slip” (eg. a lac or crush injury to the middle phalanx), then an Elson test can be performed. To do this test, flex the PIP 90 degrees over a table and have them extend against resistance. If the central slip is intact, the DIP joint will be supple. If it is ruptured, there will be weak extension of the PIP and a rigid DIP due to the action of the lateral bands.
 So, I did my hand exam… What next? Management of these injuries is often multifactorial and depends on the location of the injury, the structures involved, patient and other factors that are beyond the scope of this post. Doing a correct and detailed physical exam is the first, and most important, step in making sure a patient doesn’t walk out of the ED with an undiagnosed tendon or neurovascular injury. When practicing in the community, if you suspect that there is an associated tendonous injury based on your clinical exam, clean and repair the laceration as you otherwise would but subsequently place the patent in a dorsal blocking splint, with 15-20 wrist flexion with the hand in intrinsic plus position (MCPs at 70-90 degrees and DIP/PIP straight) and make sure they have follow-up with a hand surgeon.
So, I did my hand exam… What next? Management of these injuries is often multifactorial and depends on the location of the injury, the structures involved, patient and other factors that are beyond the scope of this post. Doing a correct and detailed physical exam is the first, and most important, step in making sure a patient doesn’t walk out of the ED with an undiagnosed tendon or neurovascular injury. When practicing in the community, if you suspect that there is an associated tendonous injury based on your clinical exam, clean and repair the laceration as you otherwise would but subsequently place the patent in a dorsal blocking splint, with 15-20 wrist flexion with the hand in intrinsic plus position (MCPs at 70-90 degrees and DIP/PIP straight) and make sure they have follow-up with a hand surgeon.
At the end of the day, it’s important to keep a high level of suspicion - a referral to a hand surgeon for a suspected tendon injury is just as valid as a referral for a definite tendon injury.
Check out these videos:
Tenodesis effect: https://www.youtube.com/watch?v=j0RBU_phUKw
Elson test: https://www.youtube.com/watch?v=wudDvOiSUlw
Generic hand exam: https://www.youtube.com/watch?v=imPQve7ZL3o
Submitted by Chris Cosgrove, MD. Ortho PGY2
Reviewed by: Daniel Osei, MD. Hand Attending
EverydayEBM Editor: Maia Dorsett (@maiadorsett)
Consultant Teaching: Tendon Injuries to the hand are often complex entities that are subject to ongoing research regarding optimal procedures for management and rehabilitation. The flexor and extensor tendon anatomy is quite complex. Both are divided into numerous “zones” created to help clarify the optimal treatment, which can vary markedly depending on injury location. Missed tendon injuries increase morbidity by complicating later management and are therefore a leading cause of malpractice claims in the world of Emergency Medicine. The most important and fundamental aspect of evaluation in these patients is a detailed hand exam. Outlined below is a guide for the evaluation and management of any patient presenting to the ED with a suspected hand injury.
Flexor Tendon Injuries
The first step is to obtain a detailed history of the mechanism of injury. Was the injury caused by a rusty farm knife or a sharp chard of glass? What was the position of the patient’s hand when the injury occurred? This is a frequently missed point to mention. You can imagine that, if the patient was lacerated with flexed fingers while gripping a knife, the location of the tendon injury itself may be in a very different location than the skin laceration when evaluating the hand in a more extended posture. Just because you can no longer see the damaged tendon in the wound doesn’t mean it’s not there.
Step 1: Observation
Evaluate the location and depth of the laceration. Look at the resting posture of the hand and the
Step 2: Passive Range of motion
These hand injuries can be really painful. A good place to start is assessment of passive motion with a maneuver that elicits the tenodesis effect. Try it on yourself - With a relaxed hand, when you passive flex your wrist, your MCP/PIP/DIP joints will extend. Similarly, wrist extension will cause passive flexion of those digits. If you passively extend the patient’s wrist and there is persistent extension of the DIP or PIP joints, you may have a flexor tendon injury in that digit.
Step 3: A detailed (ie purposeful) neurovascular exam
Flexor tendon injuries are frequently associated with neurovascular injury because of the palmar
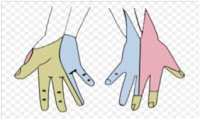 |
| Sensory territories of the hand (Source: wikipedia) |
Step 4: Flexor Tendon Exam
A quick anatomy review is necessary here because, in the hand, form truly follows function. The flexor digitorum profundus (FDP) and superficialis (FDS) tendons are both extrinsic hand muscles that power finger flexion. The FDP lies deep to FDS and then attaches distally to the distal phalanx of the 2nd-5th digits. The FDS attaches at the base of the intermediate phalanx of these digits. Why is that important to know for your physical exam? Since these muscles share a common belly and are intimately associated with one another, you must carefully isolate the desired tendon on each digit. Asking a patient to “wiggle their fingers” is an easy way to improperly assess hand function and miss isolated tendon injuries. To test the FDS: all adjacent digits must be held with all joints in extension while the patient flexes the finger at the PIP joint. To test the FDP: hold the middle phalanx in extension while asking the patient to flex just their distal phalanx. Another reason not to digital block these patients is that pain with these movements may clue the examiner into a possible partial tear or laceration.For completeness, it is also important to document motor testing for all muscles with separate nerve innervations, regardless of its proximity to the wound in question.
Extensor Tendon Injuries
Like the flexor tendons, these also can be diagnostic challenges due to the complex anatomy of the extensor mechanism. This region is comprised of extrinsic muscles that power digit extension, like the extensor digitorum communis (EDC) and an extensor aponeurosis with multiple connecting bands and ligaments. Again, a detailed history will provide valuable insight and context for your exam. Is it a result of a fight-bite injury? A crushing mechanism?
The general principles of the physical exam addressed above regarding observation, passive range of motion and a detailed neurovascular exam still apply. As diagrammed in the image above, for the dorsal hand, it is especially important to assess both the radial and ulnar nerves.
With regard to hand posture, take note if there is a resting flexed position of the digit, a mallet finger, or boutonniere deformity. This should heighten your suspicion for a tendon injury.
Assessment of the Extensor Tendon
A few important considerations are noteworthy here. First, do not be fooled by the action of the lumbricals! Remember, these muscles provide extension of the PIP and DIP joints via the lateral bands. Have the patient lay their hand flat on a table (extends the MCP joint and helps remove the influence of lumbricals) and extend at the MCP joint against resistance. Extension along an affected digit may still be possible even after complete laceration, due to the multiple contributions to the extensor mechanism. Look closely for a lack of hyperextension or differential extension in the affected finger that may be a sign an extensor tendon injury has occurred. The junctura tendinae are intertendinous fascial connections located around the MCP joint that attach tendons of the EDC and help coordinate their movements. This anatomic structure is important to keep in mind because the junctura may allow for some extension of an injured digit if the tendon injury is proximal to them.
Lastly, if you are concerned about an injury to the “central slip” (eg. a lac or crush injury to the middle phalanx), then an Elson test can be performed. To do this test, flex the PIP 90 degrees over a table and have them extend against resistance. If the central slip is intact, the DIP joint will be supple. If it is ruptured, there will be weak extension of the PIP and a rigid DIP due to the action of the lateral bands.
So, I did my hand exam… What next? Management of these injuries is often multifactorial and depends on the location of the injury, the structures involved, patient and other factors that are beyond the scope of this post. Doing a correct and detailed physical exam is the first, and most important, step in making sure a patient doesn’t walk out of the ED with an undiagnosed tendon or neurovascular injury. When practicing in the community, if you suspect that there is an associated tendonous injury based on your clinical exam, clean and repair the laceration as you otherwise would but subsequently place the patent in a dorsal blocking splint, with 15-20 wrist flexion with the hand in intrinsic plus position (MCPs at 70-90 degrees and DIP/PIP straight) and make sure they have follow-up with a hand surgeon. At the end of the day, it’s important to keep a high level of suspicion - a referral to a hand surgeon for a suspected tendon injury is just as valid as a referral for a definite tendon injury.
Check out these videos:
Tenodesis effect: https://www.youtube.com/watch?v=j0RBU_phUKw
Elson test: https://www.youtube.com/watch?v=wudDvOiSUlw
Generic hand exam: https://www.youtube.com/watch?v=imPQve7ZL3o
Submitted by Chris Cosgrove, MD. Ortho PGY2
Reviewed by: Daniel Osei, MD. Hand Attending
EverydayEBM Editor: Maia Dorsett (@maiadorsett)