A 30 y.o, woman with a history of migraines comes to the ED with diplopia
On exam she has a sixth nerve palsy on the L. Her imaging is shown below
What does she have?
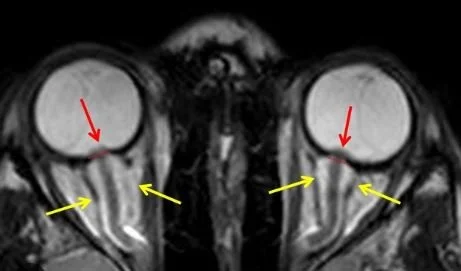
Our patient had intracranial hypertension with signs of increased intracranial pressure but without a mass or hydrocephalus Her scan shows papilledema with bulging of the optic nerves into the vitreous and dilated dural sheaths.
The condition was first described soon after the lumbar puncture was devised in 1890 by Heinrich Quincke who used lumbar puncture to treat hydrocephalus . His colleague, Max Nonne, called it pseudotumor cerebri because none of the patients presented with a brain tumor.
Two types have been identified: primary and secondary.
Primary intracranial hypertension- the most common demographic for idiopathic intracranial hypertension is obese women in their child bearing years. In true primary intracranial hypertension no other cause is found for the increase in pressure.
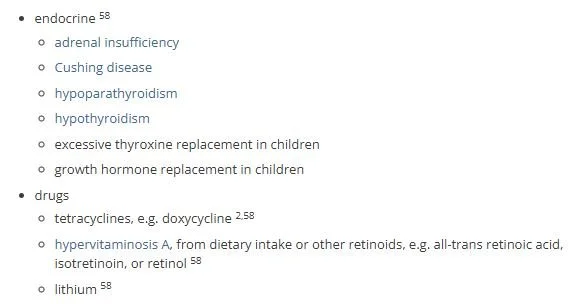
Secondary intracranial hypertension- is related to transverse sinus stenosis and jugular venous compression syndrome caused by the stylohyoid ligament. The stylohyoid ligament compresses the internal jugular vein against the C1 vertebra, leading to restricted cerebral venous outflow and increased intracranial pressure. Many other secondary causes of increased ICP have been reported as shown below. Since CSF production is responsive to steroids: low cortisol causes decreased CSF absorption and high cortisol increases CSF production by increasing sodium. Sleep apnea is also known to cause increased intracranial pressure.
SYMPTOMS
Headache- is the most common symptom. The headache worsens with bending forward and is often found in the back of the neck,

papilledema from intracranial hypertension
Pulsatile tinnitus- more than half of the cases of pulsatile tinnitus are associated with intracranial hypertension. This describes a noise heard in conjunction with the heartbeat. It can be whooshing or beating.
Signs of increased intracranial pressure- papilledema or a sixth nerve palsy are often found. Increased pressure may lead to blindness and loss of vision indicates a surgical emergency.
On imaging : a partially empty sella , flattening of the posterior globe, distension of the perioptic subarachnoid space or transverse venous sinus stenosis may be found. The patient must have a normal neuro exam except for the findings of increased intracranial
pressure in order to make the diagnosis.
On LP the pressure should be >25 to confirm the diagnosis
TREATMENT
Nearly all patients can be treated with acetazolamide to reduce CSF production. GLP-1 drugs are also given to induce weight loss. Prompt surgical intervention is necessary if vision is threatened. CSF shunting has been the standard treatment if patients are unresponsive to acetazolamide but dural venous sinus stenting is becoming increasingly common.
stenting of the transverse sinus
Because of her visual symptoms the patient underwent a spinal tap in the ED with a five inch spinal needle. The opening pressure was 40 and fluid was drained. Both her headache and diplopia resolved. She was discharged on acetazolamide.
FUN FACTS
Regardless of the cause of pulsatile tinnitus, if it can be stopped by compressing the jugular vein (which stops flow in the transverse sigmoid/jugular conduit) the noise experienced in the ear will be less if there is a stenosis. Of course compressing the jugular does INCREASE intracranial pressure.
One of the more interesting causes of secondary intracranial hypertension is an elongated styloid process or calcifies stylohyoid ligament which obstructs the jugular outside of the skull. A picture is shown below. The treatment for this is surgery.
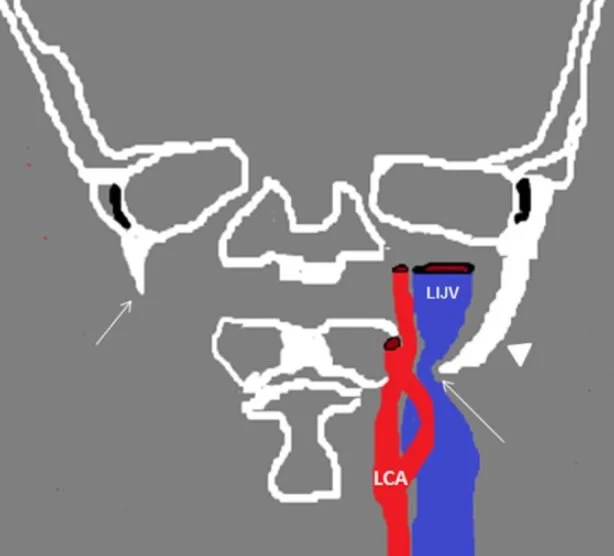
styloid hyoid obstruction is also called Eagle’s syndrome
Rizk M. Idiopathic intracranial hypertension Radiopaedia July 16 2025
Horton J. Idiopathic intracranial hypertension. NEJM 2025 ;393:1409-1419.
Higgins J, Garnett M, Pickard J, et al. An evaluation of styloidectomy as an adjunct or alternative to jugular stenting in idiopathic intracranial hypertension and disturbances of cranial venous outflow. J Neurol Surg BSkill Base 2016Nov 23;78(2):158-163.
Trivelato F, Araujo J, Siva R et al. Endovascular treatment of pulsatile tinnitus associated with transverse sigmoid sinus aneurysms and jugular bulb anomalies. Interv Neuroradiol. 2015 Aug;2194):548-551.
Kentis S, Shaw J, Kitchey L, et al. A systematic review of sleep disturbance in idiopathic intracranial hypertension, Neurol Clin Pract. 2025;15(1) :e299372
Farina R, Foti P, Pennisi I, et al. Sylo-jugular venous compression syndrome: lessons based on a case report. Am J Case Rep 2021 Aug 24;22:e932046-1-e932035-6.