A 39 y.o. woman from central Tennessee comes to the ED with fever and cough
She completed treatment for community acquired pneumonia without resolution of symptoms.
what is the next step?
Our patient had histoplasmosis. Interestingly, there is currently an outbreak of histoplasmosis around Nashville, Tennessee. 36 individuals have been reported over one month with a 30 y.o who died. This outbreak was linked to a building boom in Nashville, aerosolizing the fungus in construction areas.
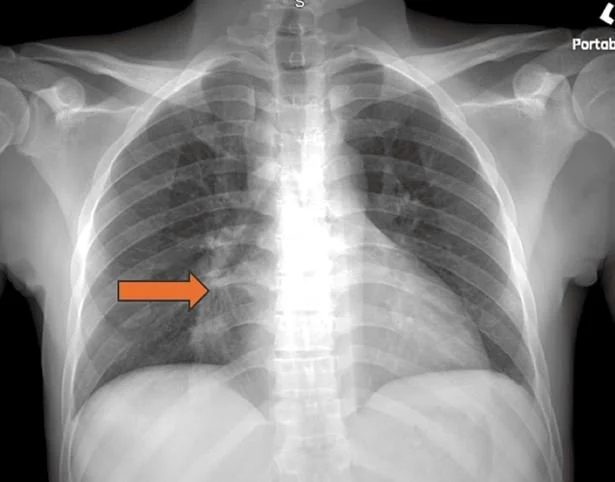
Histoplasma is a dimorphic fungus: In the soil it is filamentous, but in the body it transforms into a yeast form. These are then transported to regional nodes. A CXR of an individual with past exposure which includes most of our patients CXR often shows calcified granulomas. Yeast forms can still be present in the granulomas.

histo can mimic tuberculosis or sarcoid with granulomas and lymphadenopathy
The infection is caused by breathing in the spores of the fungus found in construction sites but most often in exposures to bird and bat droppings. The soil is enriched with nitrogen from droppings allowing the fungus to grow. Birds are not reservoirs of the fungus but bats can harbor histoplasma.

While most people are asymptomatic or have mild illness, about 10-15% of people exposed become sick with fever, cough and fatigue. This occurs anywhere from 6-18 days after exposure. Most of these are considered moderate disease and only 1% develop disseminated disease. These patients can present with ARDS, adrenal insufficiency or meningitis. Often these individuals are immunocompromised.
WHO IS AT RISK
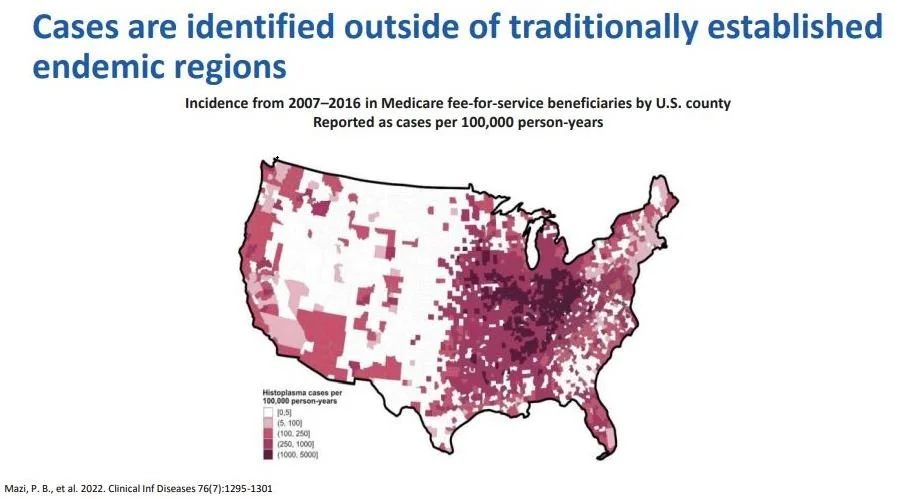
Traditionally, the fungus has been found in the Ohio and Mississippi river valleys. However, more recently it has been appearing in the western US. Risk factors used to include predominantly HIV but now autoimmune diseases lead the list at 20% of cases, cancer represents 13%, and diabetes 11%. Vacation exposures are rising and occupational exposures are rising.
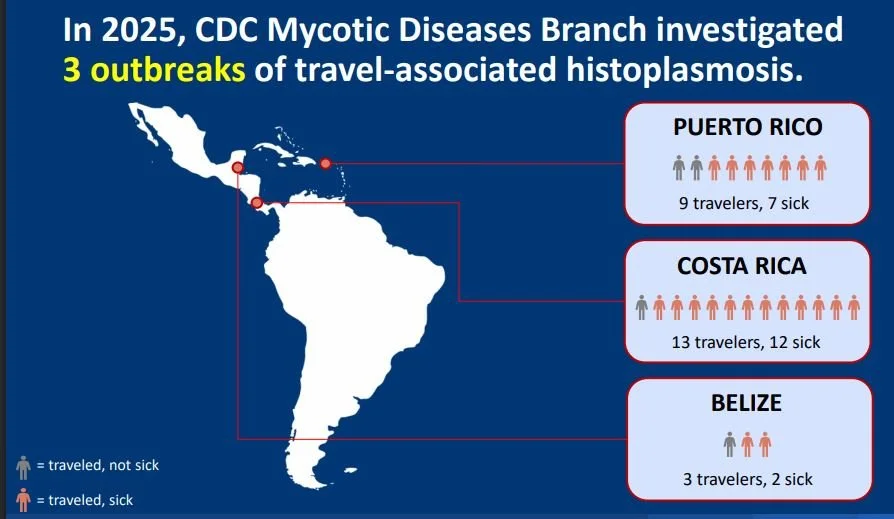
Vacation exposures-While Costa Rica is not commonly thought of as a source of histoplasmosis infection, recent studies have shown multiple infections in cavers. Often the entire group becomes ill.
Occupational exposures -histoplasmosis has been reported with constuction workers, farmers ,and guano miners. A famous case series was published in 2014 where multiple workers cleaning out tunnels filled with bat guano in the Dominican Republic became ill.
high risk areas
TESTING
The immunoassay (EIA), immunodiffusion(ID) or complement fixation (CF) are all blood tests for histoplasmosis. If any are positive, a diagnosis of pulmonary histoplasmosis can be made. Immunocompetent patients with symptoms lasting over a month should be treated. Most people do not require treatment. Because histoplasmosis tests can cross-react with blastomycosis, another soil fungus, a positive test is not always histoplasmosis although the treatment is the same.
Because the disease caused by histoplasmosis is often a flu-like illness the diagnosis t is often missed. 23-38 days is the median time until diagnosis is made by a healthcare worker with most patients being seen three times by medical professionals before the diagnosis is made. 50% receive antibiotics before the diagnosis is made.
TREATMENT
CURRENT PRACTICE GUIDELINES FOR COMMUNITY ACQUIRED PNEUMONIA DO NOT RECOMMEND TESTING FOR FUNGAL PNEUMONIAS. TREATMENT WITH ANTIBIOTICS IS RECOMMENDED FIRST.
In the immunocompetent patient consider treatment IF symptoms persist for greater than one month or symptoms are worsening. Treat with itraconazole for 6-12 weeks. In the immunocompromised treatment can be as long as one year.
FUN FACTS
Histoplasmosis can also present as skin lesions even in the immunocompetent patient.

histo can present as a skin rash even in immunocompetent patients
While most of us have been exposed, living in the Mississippi valley; you can get histoplasmosis a second time although it is usually less severe the second time and depends on the volume of spores inhaled. PPE has been shown not to be particularly effective and elimination of the source and wetting soil prior to construction have been found to be effective.
De Perio M. CDC office of communications from cave to clinic : managing histoplasmosis in returning travelers.WD5003-011526. Feb 2026 Bing Videos Maria De Perio
Akanmode A, Anwer F, Kalloo M, et al. Navigating the complexities of disseminated histoplasmosis diagnosis and management in the migrant population :a case report.Cureus 16(5):e61434.
Su C, Tazelaar HD. Histoplasma. PathologyOutlines.com website. https://www.pathologyoutlines.com/topic/lungnontumorhistoplasma.html. Accessed March 16th, 2026.
Verma S Chronic disseminated cutaneous histoplasmosis in an immunocompetent individual –a case report. International Journal of Dermatology. https://doi.org/19.1111/.)1365-4632,2996.02762.x