A 68 y.o. male comes in with epigastric pain and weakness; he has had diarrhea for two days.
what do you notice on his ekg?
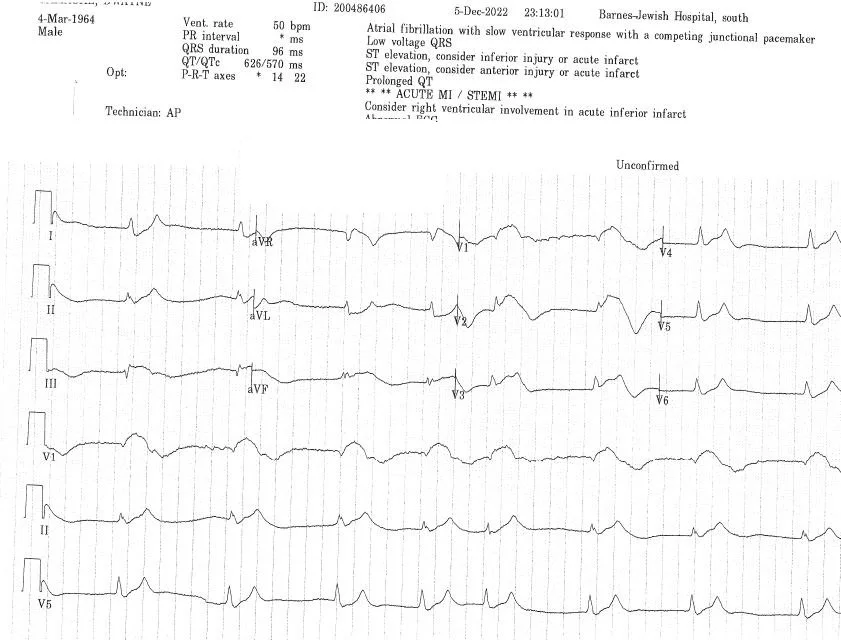
Our patient was hyperkalemic with a K of 8.5. The cath lab was activated by the ED and cardiology agreed to take him to the cath lab. When the K came back they cancelled the cath and sent him back to the ED. In spite of his diarrhea, his K was elevated because he had hepatorenal syndrome in combination with volume depletion. He had a history of cirrhosis with ascites.

consider hepatorenal syndrome in patients with spider angiomata
WHAT IS HEPATORENAL SYNDROME?
Hepatorenal syndrome, renal failure in those patients with portal hypertension and ascites .The definition of type I hepatorenal syndrome is a rise in serum creatinine of at least 0.3 mg/dL and/ or 50 % increase or greater from baseline within 48 hours, normal kidney ultrasound and bland urinalysis. In type II HRS there is a gradual decline in kidney function and refractory ascites. Estimates indicate that at least 40% of patients with cirrhosis and ascites will develop HRS in the natural history of their disease.
In HRS vasoconstriction has been shown in the renal circulation and systemic arteriolar vasodilatation in the splanchnic bed with both the renin/angiotensin and sympathetic systems playing roles. As a result systemic vascular resistance is low and there is resultant arterial hypotension. Because prostaglandins also play a role causing renal vasodilation; nonsteroidals which decrease prostaglandins should be avoided.
There is a strong association of HRS and spontaneous bacterial peritonitis. It is defined as an increase in creatinine by 50% from a stable baseline reading within 3 months.
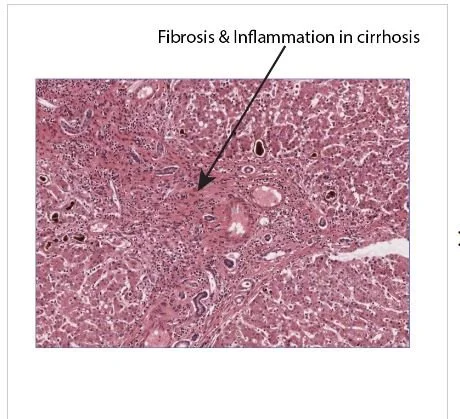
the fibrosis in cirrhosis is thought to trigger nitric oxide production causing dilation of pulmonary vessels, shunting and hypoxia. Methylene blue has been used to treat hepatopulmonary syndrome.
WHAT IS HEPATOPULMONARY SYNDROME?
Hepatopulmonary syndrome is caused by dilation of intrapulmonary vessels in patient with portal hypertension. This results in right-to-left shunting of blood and hypoxemia due to an intrapulmonary shunt. This is caused by a ventilation perfusion mismatch with more blood flowing to the alveoli in dilated vessels with preserved ventilation. This allows deoxygenated blood to return to the L heart.
The dilated vessels of the lungs are predominantly in the lower lobes and this results in orthodeoxia (worse oxygen saturation while upright) along with increased dyspnea. The findings can be confirmed by demonstration of intrapulmonary shunting when agitated saline is administered during a cardiac echo and observed in the L heart.( Normally, the agitated saline opacifies only the right heart because it is filtered by the pulmonary capillary bed but in the presence of a R to L shunt it is seen on the L side of the heart.) The only truly effective treatment for this condition is transplantation although since nitric oxide is elevated in the condition, methylene blue has been shown to increase oxygenation.
FUN FACTS
Terlipressin is a drug newly approved for treatment of hepatorenal syndrome. It selectively constricts the splanchnic vessels improving renal flow. It can also be used for esophageal varices.
Splanchnic comes from the Greek word splankhnon meaning organ. It describes blood flow to the abdominal organs.
Pulmonary capillaries which are normally 8-15 micrometers block intravenous microbubbles > 10 micrometers unless there is vasodilation of the pulmonary vessels . In the case of dilated pulmonary vessels, microbubbles appear in the L heart.
Our patient remained oliguric and on pressors for days. He was gradually weaned from pressors and his creatinine improved to 1.9 from 2.6. He was taken off diuretics and is being followed by hepatology. His K has risen to 5.5.
Krowka M, Fallon M, Kawut S, et al. International liver transplant society practice guidelines: diagnosis and management of hepatopulmonary syndrome and portopulmonary hypertension . Transplantation 2016;100;1440.
Pham D, Subramanian R, Parekh S. Coexisitng hepatopulmonary syndrome and portopulmonary hypertension: impaications for liver transplantation. J Clin Gastroenterol 2010;44:e36.
Best L, Freeman S, Sutton A, et al. Treatment for hepatorenal syndrome in people with decompensated cirrhosis: a network meta-analysis Cochrane Data Base Syst rev. 2019;9CD013103. PMID:31513287 doi:10.1002/14651858. CD013103.pub 2.