A 51 y.o. male undergoes a ventral hernia repair. that evening he develops compartment syndromes in both legs and the R arm.
What could cause this?

necrotic muscle was found

both medial and lateral compartments were opened
What could have caused his muscle necrosis and non traumatic compartment syndromes?
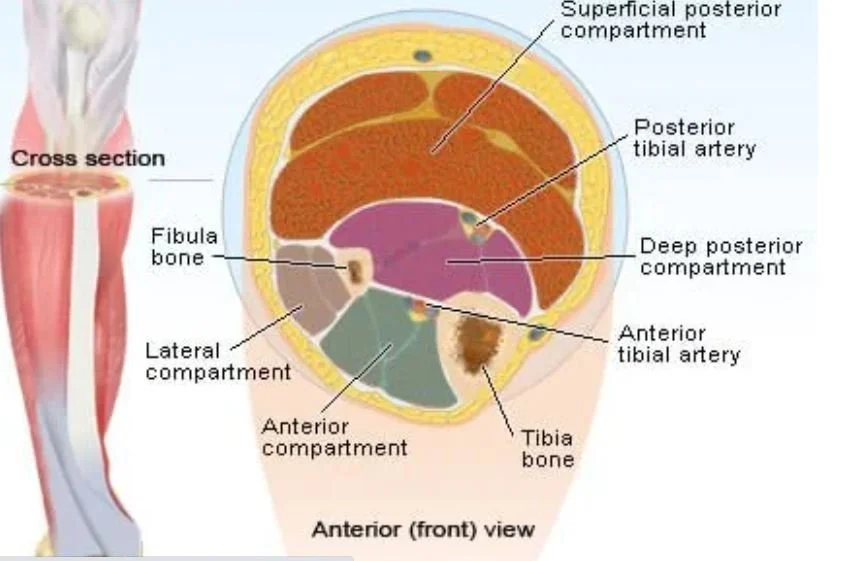
compartment syndrome usually occurs after trauma like a tibiial fracture. It can also occur after revascularization procedures where newly opened vessels cause increased pressure in a compartment with infact fascia.
1. Vascular occlusion? No abnormality venous or arterial was seen on vascular studies. No abnormalities were noted in positioning the patient which might have caused compression.
2. Hypercoagulable state? The patient had normal coags and antiphospholipid screening panel
3. Vasculitis? Rheumatoid factor, CCP, anti-HMG CoA reductase antibody were normal
4. Primary muscle disease? A muscle biopsy was done which showed just necrotic muscle with fibroblast infiltrate. A complete myopathy panel showed the patient’s IgG weakily binds to PM-Scl 75 which makes this borderline positive for scleroderma but the patient had no ulcers or signs of scleroderma..
So the two more likely diagnoses here are neuroleptic malignant syndrome from droperidol or malignant hyperthermia from general anesthesia.
5. Neuroleptic malignant syndrome? Serotonin syndrome? The pt had received droperidol prior to development of his muscle necrosis. Neuroleptic malignant syndrome is most often associated with antipsychotics or antiemetics. Central dppamine receptor blockage is thought to be the cause of NMS and blockage of dopamine in the hypothamus results in hyperthermia. Blockage of dopamine in the nigrostriatal pathways leads to rigidity and tremor. Patients often present with altered mental status. Was his “muscle stiffness” part of neuroleptic malignant syndrome? It was felt to be too delayed.
Serotonin syndrome can look similar to NMS but often has hyperreflexia (clonus) and diaphoresis.



6. Malignant hyperthermia? This is a disorder of skeletal muscle metabolism that may be triggered by general anesthetic agents like succinylcholine. Every anesthetic agent has been implicated. It has been reported to cause severe muscle fiber contraction and compartment syndrome. In some cases there are genetic predisposition in families with RYR1 and CACNA1S genes but it is not known what triggers most cases. A definitive test can now be performed on muscle where a live muscle biopsy and caffeine-halothane contracture test is performed. If the muscle contracts it is considered positive.
A sample of our patients muscle was sent to the Mayo Clinic for performance of muscle testing.
Volpi-Abadie J, Kaye A, Kaye A. Serotonin syndrome. Ochsner J. 2013 Winter; 13(4):5333-540.
Johnson I, Andrezejowski J, Currie J. Loer limb compartment syndrome resulting from malignant hyperthermia. Anaesth Intensive Care 1999;27:292-294.
Osman B, Saba I, Watson W. A case report of suspected malignant hyperthermia; how will the diagnosis affect a patient’s insurability. Case Reports in Anesthesiology 2018;65:3821.
Choke E, Sayers R, Born M. Compartment syndromes Mechanisms of Vascular Disease: A Reference Book for vascular Specialists.
Sayar U, Ozer T, Mataraci I. forearm compartment syndrome caused by reperfusion injury. Case Rep Vac Med 2014;2014:931410