A 49 y.o. male presents with several months of hoarseness
His CT scan shows bilateral vocal cord infiltration with no nodes enlarged.

What is the differential for vocal cord infiltration?
Our patient had bilateral infiltration of the vocal cords with vocal cord paralysis. His presentation was hoarseness which is the reason for 1% of all visits to primary care physicians. Vocal cord paralysis is present in 2.8-8% of the cases. This represents a more serious condition and laryngoscopy is recommended to rule it out.
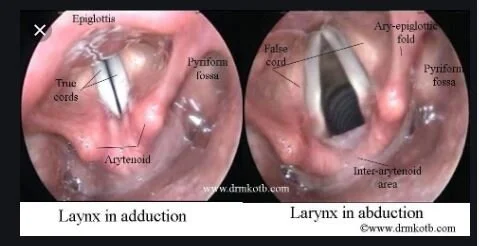
anatomy of the arytenoids and cords
While the prevalence of rheumatoid arthritis is 1% in the population at large, up to 88% in postmortem studies have laryngeal involvement of the cricoarytenoid joint. Other conditions which can causing dysfunction in the cricoarytenoid joint are listed below:
Gout
Syphilis
Gonorrhea
Sarcoid, amyloidosis, lyme disease, lupus, wegener’s, lymphoma, and tuberculosis can cause laryngeal involvement as well. Neuropathy from diabetes may cause vocal cord dysfunction and reflux disease may also cause bilateral vocal cord immobility. If no cause is found for vocal cord immobility a CT of the entire course of the vagus nerve is recommended.

the cricoarytenoid joint is the axis around which the cords pivot
In the case of our patient a biopsy was done showing squamous cell carcinoma.
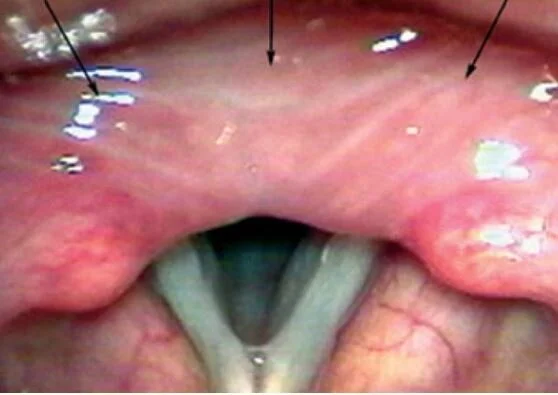
Edema of the intraarytenoid space may occur as in this case in RA.
Berterud A. Rheumatoid arthritis in the larynx. Scand J Rheumatol. 1991;20:215. Doi: 10.3109/03009749109103025.
Ramos H, Pillon J, et al. Revista Brasiliera fe Otorrinolaringolgia. Rev. Bras. Otorrinolaringol.2004 Vol 71(4)
Reiter R, Hoffmann T, Pickhard A, Brosch S. Hoarseness—causes and treatments. Dtsch Arztebl Int. 2015 May;112(10):329-237. Doi: 10.3238/arztebl 2015.0329
Kamanli A, Gok S. Sahin I et al. Bilateral cricoarytenoid joint involvement in rheumatoid arthritis: a case report 2001 Rheumatology, vol 40,(5), 593-594.
Fried MP, Sharpiro J. Acute and chronic laryngeal infections. In: Paperella MM, Shumrick DA, Gluckman J, Meyerhoff W, eds. Otolaryngology, edn 3. Philadelphia : W.B. Saunders, 1991:2245-56.