If There's a Delay, Consider TXA: On Anti-fibrinolytic Therapy for Management of Aneurysmal Subarachnoid Hemorrhage
Clinical Scenario: While working in a community emergency department you see a middle aged otherwise healthy female who developed a thunderclap headache two hours ago while lifting weights. She is very nauseated, has intermittent vomiting, but is able to respond to your questions. An emergent Head CT shows subarachnoid hemorrhage involving the suprasellar, interpeduncular, and ambient cisterns with associated ventriculomegaly. You call the neurosurgeon at the closest tertiary care hospital and he asks whether you considered giving tranexamic acid (TXA) prior to transport.
Clinical question: Does TXA improve outcomes for patients with spontaneous subarachnoid hemorrhage? Does it increase the risk for thrombotic event/stroke?
Literature Review:
In people who suffer from aneurysmal subarachnoid hemorrhage, rebleeding is a cause of significant death and disability, peaking in incidence 24 hrs from the initial presenting event [1]. More than a third of rebleeding events occur within 3 hrs and more than half within 6 hrs [2]. It is thought that part of the mechanism of rebleeding is dissolution of the clot at the site of the aneurysm. While securing the aneurysm via coiling or clipping is the standard of care to prevent rebleeding, in instances where there is an delay of care is unavoidable, it was been postulated that anti-fibrinolytic therapy, which may mitigate this process, may decrease the incidence of rebleeding.
One form of anti-fibrinolytic therapy is TXA, a synthetic analog of the amino acid lysine that works as a hemostatic agent by binding to the lysine binding sites on plasminogen, thereby competitively inhibiting its conversion to plasmin and subsequently fibrin degradation. Existing studies suggest that TXA decreases bleeding in menorrhagia and cardiopulmonary bypass, as well as to improves mortality in trauma patients dying of massive hemorrhage [3,4,5,6]. Does this hemostatic benefit apply to spontaneous subarachnoid hemorrhage?
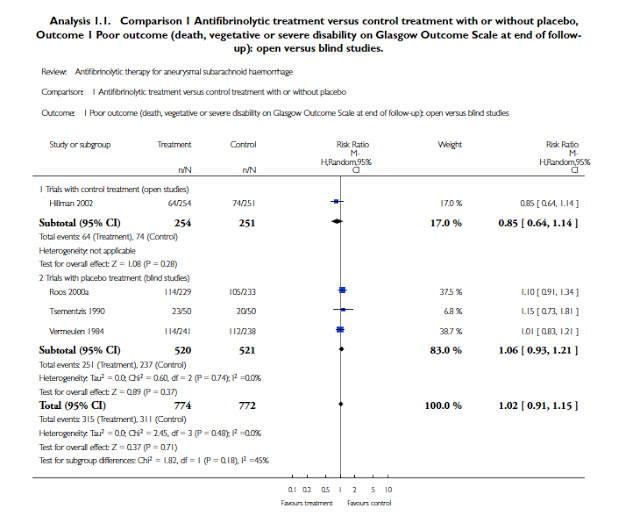
A large number of studies regarding anti-fibrinolytic therapy for aneurysmal subarachnoid hemorrhage have been published. These were assessed in a 2013 Cochrane meta-analysis aimed at addressing the overall clinical effects of such therapies on rates of rebleeding and overall morbidity/mortality in aneurysmal SAH [7]. This was prompted in part because of concern that even if antifibrinolytics decreased risk of rebleeding, this would be offset by an increased risk of cerebral ischemia, which tends to develop between 4-14 days after initial SAH. The Cochrane review included only randomized trials that compared antifibrinolytic to placebo vs. control and assessed subsequent outcomes on an intention to treat basis. Their systematic review included 10 studies [with a pooled patient sample of 1904 who received TXA, 597 placebo, and 348 control]. Nine of these studies used TXA as the antifibrinolytic agent and one used epsilon-amino-caproic acid (39 patients). These studies were extremely heterogeneous in their anti-fibrinolytic treatment regimens. One study treated for less than 72 hrs (before onset of potential cerebral ischemia) [8] and others treated up to six weeks (through peak time of cerebral ischemia). Two of the studies concurrently treated patients with therapy (such as nimodipine) to reduce the risk of cerebral ischemia [8,9]. Their analysis found that that TXA did not affect the overall morbidity (risk of poor outcome was RR 1.02; 95% 0.91-1.15) or mortality (death from all causes RR 1.00; 95% CI 0.85-1.18). Administration of TXA did decrease the risk of rebleeding (RR 0.65, 95% CI 0.44 to 0.97; 78 per 1000 people), but this was offset by the increased the risk of cerebral ischemia (RR 1.41, 95% CI 1.04 to 1.91; 83 per 1000 people).
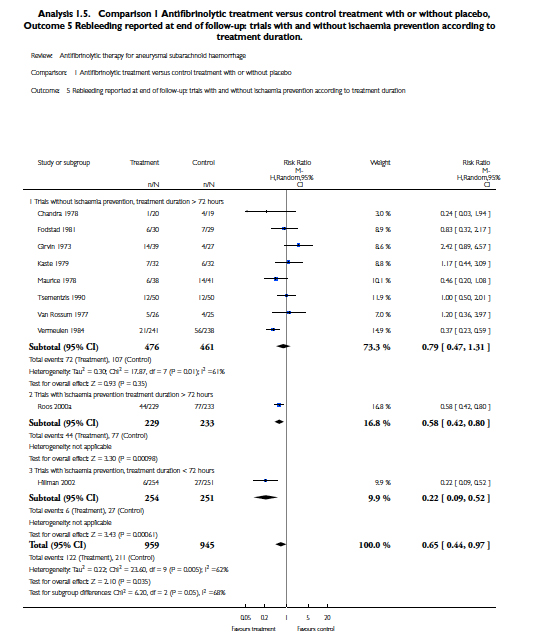
There was was considerable heterogeneity between the older studies and the newer studies, which may be attributed to newer studies using specific treatments to prevent the risk of cerebral ischemia.
While this overall analysis suggests that TXA may not significantly benefit long term outcome in aSAH, the majority of the studies administered the drug for a prolonged period time of > 10 days, at which point definitive aneurysmal treatment via endovascular or surgical intervention should be achieved. One study examined short term (mean of 15.3 +/- 16 hrs) use of an anti-fibrinolytic therapy (E-Aminocaproic acid - EACA) on risk of rebleeding, mortality and favorable neurologic outcome at 3 months [10]. They prospectively studied 248 patients with aSAH. Patients were not randomized, but the two groups were similar with regard to baseline characteristics predictive of rebleeding risk and neurologic outcome, including anticoagulation and Hunt-Hess grade (with the exception of blood pressure which was not assessed). The authors compared the outcomes of 73 patients who received EACA with those of 175 patients who did not. They found that there was a significant decrease in rebleeding in EACA-treated patients (2.7% vs. 11.4%), as well as a general trend towards favorable neurologic outcome in those who received anti-fibrinolytic therapy. While we will continue to await randomized, placebo-controlled trials to determine if (and which) antifibrinolytic therapy improves outcome for patients with aSAH, the AHA/ASA guidelines have incorporated anti-fibrinolytic therapy into the recommendations for medical measures to prevent rebleeding [2]:
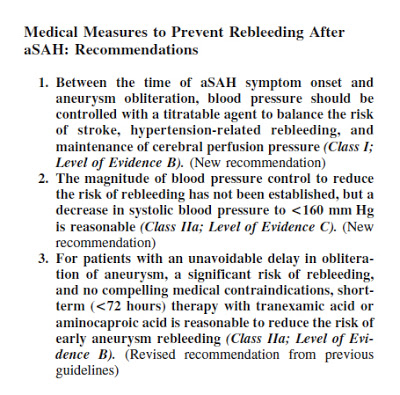 |
| Current AHA/ASA Guidelines for Medical Management to Prevent Rebleed in Aneurysmal SAH (Ref 2) |
Take home: TXA may reduce the risk of rebleeding in aneurysmal subarachnoid hemorrhage, but current evidence does not strongly support a benefit regarding survival or morbidity. In studies using prolonged anti-fibrinolytic therapy, the benefit conferred by decreased risk of rebleed was offset by increase in cerebral ischemia. However, more recent trials of short-term antifibrinolytic therapy have had promising, but far from definitive results. Current AHA/ASA guidelines encourage its use for patients who will have a delay in aneurysm obliteration.
Submitted by Melissa Kroll, PGY-3
Edited by Maia Dorsett, PGY-4
Faculty Reviewed by Peter Panagos
References
1.Guo, L. M., Zhou, H. Y., Xu, J. W., Wang, Y., Qiu, Y. M., & Jiang, J. Y. (2011). Risk factors related to aneurysmal rebleeding. World neurosurgery, 76(3), 292-298.
2. Connolly, E. S., Rabinstein, A. A., Carhuapoma, J. R., Derdeyn, C. P., Dion, J., Higashida, R. T., ... & Vespa, P. (2012). Guidelines for the management of aneurysmal subarachnoid hemorrhage a guideline for healthcare professionals from the American heart association/American stroke association. Stroke, 43(6), 1711-1737.
3. Jimenez, J. J., Iribarren, J. L., Lorente, L., Rodriguez, J. M., Hernandez, D., Nassar, I., ... & Mora, M. L. (2007). Tranexamic acid attenuates inflammatory response in cardiopulmonary bypass surgery through blockade of fibrinolysis: a case control study followed by a randomized double-blind controlled trial. Crit Care, 11(6), R117.
4. Lethaby, A., Farquhar, C., & Cooke, I. (2000). Antifibrinolytics for heavy menstrual bleeding (Cochrane Review). The Cochrane Library, (4).
5. Williams-Johnson, J. A., McDonald, A. H., Strachan, G. G., & Williams, E. W. (2010). Effects of tranexamic acid on death, vascular occlusive events, and blood transfusion in trauma patients with significant haemorrhage (CRASH-2) A randomised, placebo-controlled trial. The West Indian medical journal, 59(6), 612-624.
6. Morrison, J. J., Dubose, J. J., Rasmussen, T. E., & Midwinter, M. J. (2012). Military application of tranexamic acid in trauma emergency resuscitation (MATTERs) study. Archives of surgery, 147(2), 113-119.
7.Baharoglu, M. I., Germans, M. R., Rinkel, G. J., Algra, A., Vermeulen, M., van Gijn, J., & Roos, Y. B. (2013). Antifibrinolytic therapy for aneurysmal subarachnoid haemorrhage. The Cochrane Library.
8.Hillman, J., Fridriksson, S., Nilsson, O., Yu, Z., Säveland, H., & Jakobsson, K. E. (2002). Immediate administration of tranexamic acid and reduced incidence of early rebleeding after aneurysmal subarachnoid hemorrhage: a prospective randomized study. Journal of neurosurgery, 97(4), 771-778.
9.Roos, Y. B. W. E. M., & STAR Study Group. (2000). Antifibrinolytic treatment in subarachnoid hemorrhage A randomized placebo-controlled trial. Neurology, 54(1), 77-77.
10. Starke, R. M., Kim, G. H., Fernandez, A., Komotar, R. J., Hickman, Z. L., Otten, M. L., ... & Connolly, E. S. (2008). Impact of a protocol for acute antifibrinolytic therapy on aneurysm rebleeding after subarachnoid hemorrhage. Stroke, 39(9), 2617-2621.