A 61 y.o. woman with a history of diabetes, HT and remote history of opiod use disorder presents with abdominal pain, nausea and vomiting over one day.
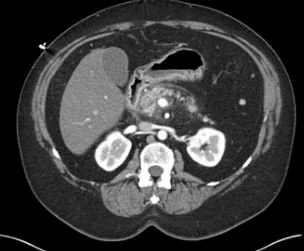
A CT was done
Vitals showed T 36.6 BP 84/68 HR 111 SpO2 97%
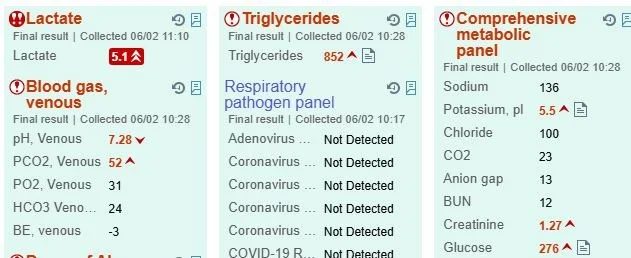
After hydration, a lipid panel showed triglycerides of 1681. what are you concerned about?
Our patient has acute severe pancreatitis fulfilling the three diagnostic criteria of epigastric pain, elevated lipase and imaging consistent with pancreatitis. She had marked hypertriglyceridemia. After ethanol and gallstones, hypertriglyceridemia is the third leading cause of acute pancreatitis, accounting for 4% of the cases. It can occur during infusion of lipid emulsions for parenteral feeding, or the use of propofol which is infused in a 10% fat emulsion.
Hypertriglyceridemia can be attributed to either primary or secondary causes. Primary causes ( caused by a single gene mutation) include familial dyslipidemias such as familial chylomicronemia. These often result in severe hypertriglyceridemia (>1000 mg/dL). Secondary causes include being overweight, excessive alcohol consumption, uncontrolled diabetes mellitus, hypothyroidism and medications such as estrogens, corticosteroids, and retinoids. These secondary causes are less likely to cause high triglycerides.
It is estimated that 1 in 600 individuals has a genetic predisposition to hypertriglyceridemia which is not the familial type affecting the lipoprotein lipase gene but is polygenic; affecting several lipid regulating genes.
The SHIBA(severe hypertriglyceridemia influenced by alcohol) syndrome has been described. Acute heavy alcohol intake with a fatty meal increases chylomicrons in the small intestine. They are taken to the liver resulting in an upregulation of microsomal triglyceride transfer protein(MTP) creating very low density lipoproteins(VLDL). These VLDL proteins carry chylomicrons from the liver to the rest of the body.
Chylomicrons are believed to be responsible for pancreatic inflammation by impairing circulatory flow in capillary beds resulting in ischemia. This ischemia triggers necrosis, edema and inflammation. Necrosis can be seen on CT.
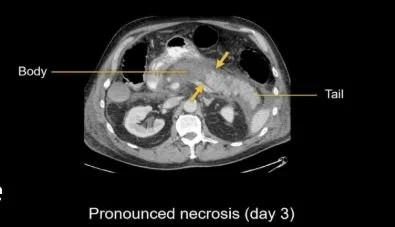
pancreatic necrosis appears as a hypodense area. Tumors can also cause pancreatitis
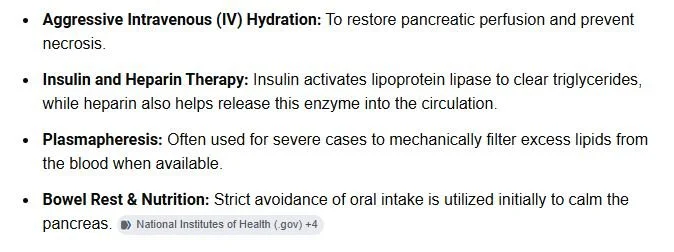
TREATMENT OF PANCREATITIS
In addition to alcohol, clozapine, olanzapine and steroids should be avoided.
FUN FACT
Pseudo hyponatremia can result from high triglycerides but rather than treat the sodium, the triglycerides should be treated aggressively.
Our patient was hydrated and given pain meds. Because her triglycerides continued to rise she was admitted to the ICU, put on an insulin drip and considered for plasmapheresis. Her severe pancreatitis was thought to be due to a combination of factors including familial history of cholesterolemia, diabetes and alcohol. She underwent one session of plasmapheresis and an insulin drip with improvement. Fenofibrate was added to her atorvastatin.
Feingold KR, Adler RA, Ahmed SF, et al., editors Endotest. 2025. Pancreatitis secondary to hypertriglyceridemia.South Dartmouth (MA) https://www.ncbi.nlm.nih.gov/books/NBK279082/
Grigore M, Valaban D, Jinga M, et al. hypertriglyceridemia-induced and alcohol-induced acute pancreatitis-a severity comparative study Diagnostic(Basel)2025 Apr 1;15(7):882.
Nwaobi S, Khan A, Ejemolon P, et al. a case of hypertriglyceridemia-induced actue pancreatitis in the setting of alcohol abuse. Cureus. 2023 Apr 23;15(4):e38028.
Nwaobi S, Khan A, Ejemolon P, et al. a case of hypertriglyceridemia-induced actue pancreatitis in the setting of alcohol abuse. Cureus. 2023 Apr 23;15(4):e38028.
Acute pancreatitis and hypertriglyceridemia. Lindberg DA. Gastroenterol Nurs. 2009;32:75–4. doi: 10.1097/SGA.0b013e31819de3e0.
Dron J, Hegele R. Genetics of hypertriglyceridemia Front Endocrinol(Lausanne)2020 Jul 24;11:455.khg