A 30 y.o. male comes to the ED with erectile dysfunction . He has noted a change in the color of his urine intermittently.

The sample on the R is from yesterday and the one on the R is from today.
What would be important to see under the microscope?
The first step in the evaluation of the patient would be to look at the urine under a microscope. If no RBCs are present and the urine still contains hemoglobin, hemolysis should be considered. Urine is concentrated overnight and hemolysis would be most visible in an early morning sample. The other possibility would be myoglobin which turns the urine dark from muscle damage since heme is released. The way to tell the difference is to look at the serum. In myoglobinuria, the serum will be clear and in hemolysis, the serum will be pink
Knowing the patient has erectile dysfunction with hemolysis suggests paroxysmal nocturnal hemoglobinuria (PNH) which was his diagnosis. More than 50% of patients with PNH have erectile dysfunction.
It is a form of hemolysis caused by unopposed complement activation leading to bone marrow failure. The PIGA gene in STEM cells in the marrow mutates to cause abnormal cells to form. These cells lack the complement regulatory proteins CD55 and CD59 and these cells cause the body to recognize healthy RBCs as damaged. Since complement is unopposed and without normal protective proteins keeping complement in check, general hemolysis results.
PNH is a difficult diagnosis to make because it often presents with just fatigue, and it can be very mild. Fewer than 40% of PNH patients who present with hemoglobinuria are diagnosed in 12 months after numerous physician interactions. The spectrum of disease includes classic hemolytic PNH which our patient had, PNH associated with bone marrow failure as in myelodysplastic syndromes, and aplastic anemia. The major findings are:
1. Hemolysis
2. Hemoglobinuria
3. Smooth muscle dystonia- Free hemoglobin in the serum acts as a scavenger of nitric oxide and its depletion results in severe muscle contractions in the chest and abdomen. Dysphagia and erectile dysfunction are also found. Both vasospasm from a lack of nitric oxide and smooth muscle spasms contribute to erectile dysfunction.
4. Thrombosis- Depleted nitric oxide also causes endothelial dysfunction leading to thrombosis. The main cause of death in individuals with PNH is thrombosis.
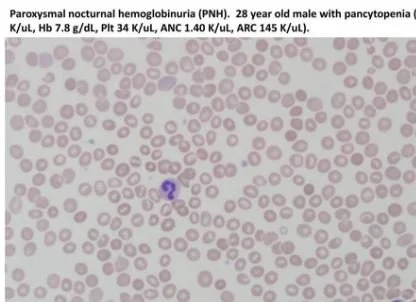
smear of PNH with pancytopenia
DIAGNOSIS
LDH may be elevated in hemolysis. Low haptoglobin and high indirect bilirubin also occur with hemolysis . The definitive diagnosis is made by low cytometry which identifies cells lacking certain proteins. (CD55 and CD59) These are proteins which would limit the destructive effects of complement.
Unlike thrombotic microangiopathies (TTP/HUS), where schistocytes are numerous, their presence in PNH is uncommon. They are sometimes found but often linked to the intense hemolytic process. Severe hemolytic events in PNH can be triggered by exercise, infection or stress.
TREATMENT
Since PNH is caused by unopposed complement; complement inhibitors are used to treat it.
Complement inhibitors include eculizumab which inhibits complement activation at C5 , In severe cases blood transfusions are needed. In the most extreme cases stem cell transplants are needed.
FUN FACTS
Sickle cell disease and banked blood also cause hemolysis, thrombosis and vaso-occlusion similar to PNH. Studies are underway using nitrous oxide as a treatment for sickle cell vasooclusive crises for this reason. So far, results have been mixed.

results of finasteride
There is a recent craze involving the use of finasteride to prevent hair loss in men. It can delay hair loss for up to ten years. Unfortunately, since it blocks dihydrotestosterone it often leads to erectile dysfunction and ejaculatory issues. It is vastly more common than PNH as a cause of erectile dysfunction.
Kokoris S, Polyviou A, Evangelitdis P et al. Thrombosis in paroxysmal nocturnak hemoglobinuria: from pathogenesis to treatment. Int J Mol Sci. 204Nov 11;25(22):12104.
Parker C., Omine M., Richards S., Nishimura J.-I., Bessler M., Ware R., Hillmen P., Luzzatto L., Young N., Kinoshita T., et al. Diagnosis and Management of Paroxysmal Nocturnal Hemoglobinuria. Blood. 2005;106:3699–3709. doi: 10.1182/blood-2005-04-1717.
Keating S, Machdhhar R, Jain U, et al. An interesting case of paroxysmal nocturnal hemoglobinuria with renal involvement. Cureus 2024. DOI: 10.7759/cureus.63917
Kahn M, Maley J, Lasker G, et al. Updated role of nitric oxide in disorders of erythrocyte
Published in final edited form as: Cardiovasc Hematol Disord Drug Targets. 2013 Mar 1;13(1):83–87. doi: 10.2174/1871529x11313010009