A 43 y.o. truck driver is referred to the ED for a posterior shoulder dislocation and possible seizure.
what do you notice on his head CT?

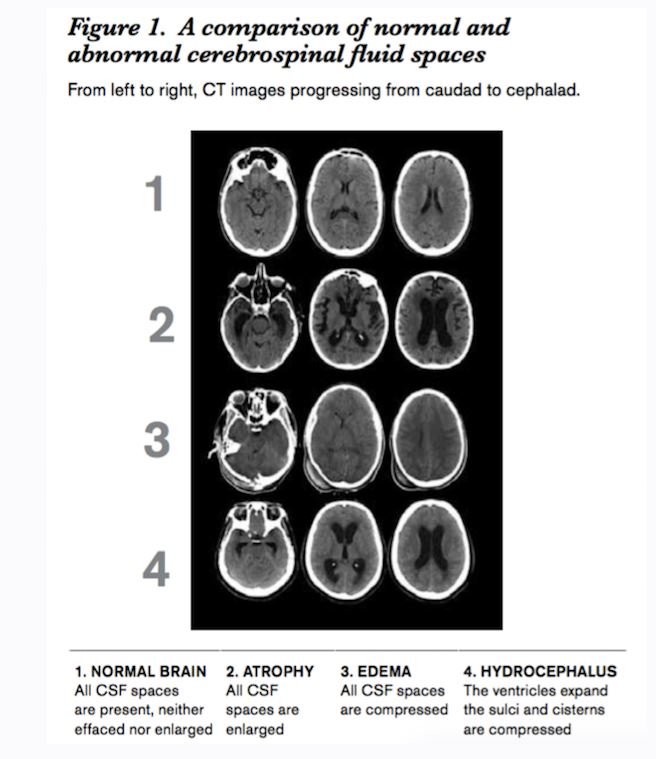
compare it to the normal CT of a young person below

Our patient had increased intracranial pressure from malignant hypertension. The ventricles are very small and sulci are effaced. He had altered mental status but DO NOT DO AN LP IF YOU SUSPECT INCREASED INTRACRANIAL PRESSURE.
While some individuals have survived an LP with increased ICP, there is a serious potential for herniation. Herniation has been reported in patients with acute bacterial meningitis during LP (there have even been cases of spontaneous herniation without performing an LP)
Our patient had altered mental status. This and also seizure within a week of presentation are two reasons the Infectious Diseases Society of American recommends CT before LP. When his CT showed increased ICP, efforts were made to bring his BP down with nicardipine, shoulder relocation was postponed and the pt was admitted to the ICU.

While we tend to look at the brain parenchyma for pathology; the csf spaces can be equally useful in detecting pathology. With brain atrophy all CSF spaces are enlarged. In hydrocephalus the ventricles are enlarged and the sulci and cisterns are compressed.
Our patient was treated for his hypertension in the ICU. MRI showed scattered lesions in the periventricular white matter consistent with acute infarcts. These findings are consistent with small vessel diease, vasculitis or autoimmune etiologies like Susac syndrome. Susac syndrome is is thought to be an immune mediated process of endothelial necrosis which leads to microinfarcts of the brain, retina and cochlea(causing deafness).
Ophthalmology evaluated the patient and the exam of the retina was normal except for cotton wool spots. It was decided after ruling out all other causes for his strokes; his presentation was due to malignant hypertension. His broken, posteriorly dislocated shoulder was repaired in the OR and his BP was controlled. He is doing well after discharge.

branch retinal artery defects in young patients without atherosclerosis are characteristic of Susac”s syndrome.
Salazar L, Hasbun R. Cranial imaging before lumbar puncture in adults with community-acquired meningitis: clinical utility and adherence to the Infectious diseases Society of America Guidelines. Clin Infect Dis 2017 Jun 15:64(12):1657-1662.
Greco A, De Virgillio A, et al. Susac”s syndrome--pathogenesis , clinical variants and treatment approaches. Autoimmun Rev 2014;13(8):814-821.
Hale L, Weaver M, Shah R, et al. Can’t hear, can’t think, can’t see what can this be? Medical Retina . 2018 Jan/Feb:33-38