A 52 y.o. woman who is on chronic steroids for asthma presents with HA x one month. She recently noted polyuria and polydipsia.
Prolactin is 83.2 and cortisol is 1.7.

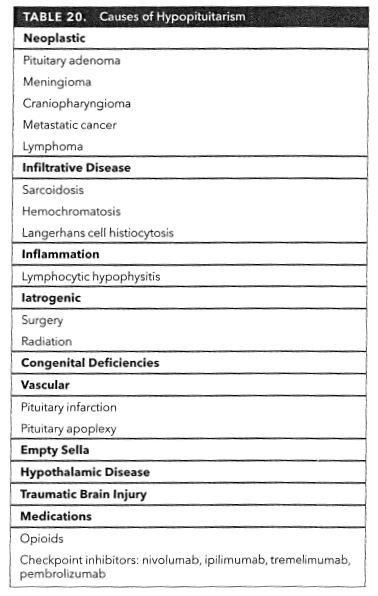
she has a mass in the sella on MRI. What could it be?

: this is a review of the anatomy; the cavernous sinuses are shown in blue.
Our patient had a pituitary enlargement. . She had a mass extending into the cavernous sinuses along the medial aspect of the internal carotid. This caused central diabetes insipidus.
She had three problems
1. High prolactin caused by loss of dopamine due to compression of the pituitary stalk by what was initially thought to be a non functioning pituitary adenoma. Her prolactin was 83.2. The most common cause of hyperprolactinemia is pregnancy, not tumor. The most common cause of medication related hyperprolactinemia are antipsychotics which also block dopamine.
2. ADH deficiency ( central diabetes insipidus) was diagnosed because of lack of adequate urine Osm concentration on water deprivation. the pituitary enlargement was responsible for ADH deficiency causing diabetes insipidus because ADH made in the hypothalamus is not delivered to the pituitary because of tumor compression of the stalk and posterior pituitary.
3. Adrenal insufficiency was due to chronic steroid use with a cortisol of 1.7.
Most central diabetes insipidus is not caused by a tumor, but by autoimmune hypophysitis( enlargement of the pituitary and stalk). This can be the result of IgG4 disease, drugs like nivolumab, Wegeners or antibodies to vasopressin producing cells. It can also be caused by infiltrative diseases like sarcoid or hemochromatosis . Trauma, whether TBI or surgical, can also cause DI.
In contrast to our patient, some pituitary tumors produce hormones directly. In acromegaly growth hormone is produced causing longitudinal growth which results in gigantism. Tumors which secrete hormones are often treated with surgery and radiation.

Robert Wadlow was born in Alton Illinois and grew to over 8 foeet due to growth hormone excess from a pituitary tumor.
The treatment for her diabetes insipidus was desmopressin 100 mg replacing the vasopressin she lacks and her adrenal insufficiency was treated by tapering her chronic steroids. She is scheduled to be followed by endocrine. She seen by endocrine in clinic she was found to be on dupilumab which is a monoclonal antibody.. Endocrine felt this may be responsible for hypophysitis . It is not yet determined if her pituitary enlargement is related to an adenoma or immune process.

Bleeding from a pituitary tumor into the optic chiasm is a surgical emergency.
Giacomozzi C, Nicoli L , Sozzi C. Case report: lipoma of the tuber cimerei, mimicking a pituitary gland abnormality in a girl with central precocious puberty. Oct 11; 2021. 12:766253https:doi.org/10.3389/fendo 2021.765253
Skinner D. Rethinking the stalk effect: a new hypothesis explaining suprasellr tumor-induced hyperprolactinemia, Med Hypotheses 2009 Mr; 72(3):309-310.
Khan C,Khab Suheb K, Radbel J. Diabetes Insipidus . StatPeals (internet)
Watson F, Austin P,(2021-10-01) Physiology of human fluid balance Anaethesia & Intensive care 22(10):644-651 doi:10.1016)/mpaic 2021 07.020
MKSAP 19 ISBN:978-1-938245-76-6