A 44 y.o. male fell down a flight of stairs. He landed on the L knee, stood up and fell on to the R knee.
What do you see on the xrays?


you can compare it to the R knee
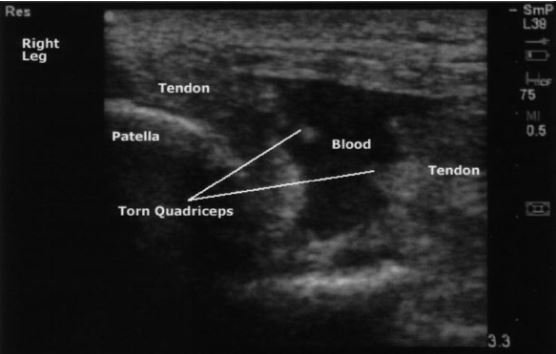
Our patient had bilateral patellar quadriceps tendon ruptures. A knee effusion is visible on the L and not on the R knee and the patella is higher riding on the left . He had significant swelling of the L knee and was unable to walk. . The usual circumstance causing the injury is that the quadriceps muscles contracts with the knee in a flexed position. Risk factors for quadriceps tendon rupture include underlying inflammation as in lupus, chronic renal disease, diabetes or chronic steroid use. Quadriceps tendon rupture is three times more likely than patellar tendon rupture. Patellar tendon rupture Is more common under age 40.

Ultrasound is the easiest way to make the diagnosis since patients often have significant swelling and pain. As in the case of our patient he could not stand and this significantly delayed his xrays.
There are several other knee injuries that can be easily missed on plain xray.
Knee dislocation- these can be difficult to diagnose if there is no neurovascular injury and they reduce spontaneously prior to presentation. Anterior dislocations are the most common and usually occur during forced hyperextension. They are more common in morbidly obese patients.
Tibial plateau fx- these are commonly missed because the fragment can overlie normal bone. It is caused by the femur impacting the tibia.

a 16 y.o. soccer player with a tibial plateau fracture.
Avulsion of the proximal fibular head- the arcuate sign can be a clue to the injury. This is a small fracture of the fibula associated with and ACL injury.

PEARL:
When possible, test the injured knee for knee extension. Xrays can be normal with a ruptured quadriceps tendon. In this case the xray was read as knee effusion on the L and normal on the R. Beware of other subtle knee injuries.
Our patient was diagnosed on ultrasound and taken to surgery. He underwent repair of both R and L quadriceps tendons.
LaRocco B, Zlupko G, Sierzenski P. Ultrasound diagnosis of quadriceps tendon rupture. J of EM 2008 vol 35(3) 293-295.
Strub W. The arcuate sign Radiology 2007 Vol 244(2) https://doi.org/10.1148/radiol.2442042160
McKee L, Ibrahim M, Lawrence T,et al. Current concepts in acute knee dislocation: the missed diagnosis?Open Ortho J. 2014;8:162-167.
Maheshwan J, Pandeey V, Mhaskar V. Anterior tibial plateau fracture: an often missed injury. Indian J Orthop. 1014 Sep-Oct ;48(5):507-510.
Do K, Zakaria A, Bertasi T, et al. A Schatzker type III tibial plateau fracture in a soccer player: a case report . Cureus 15(7):e42015.doi:10.7759/cureus. 42015