A 40 woman was run over by her own truck 5/2 and returns 5/23 with swelling of the thighTh
She had sustained a sacral and pelvic fx initially but no fx of the femur

hint: there is no femur fracture
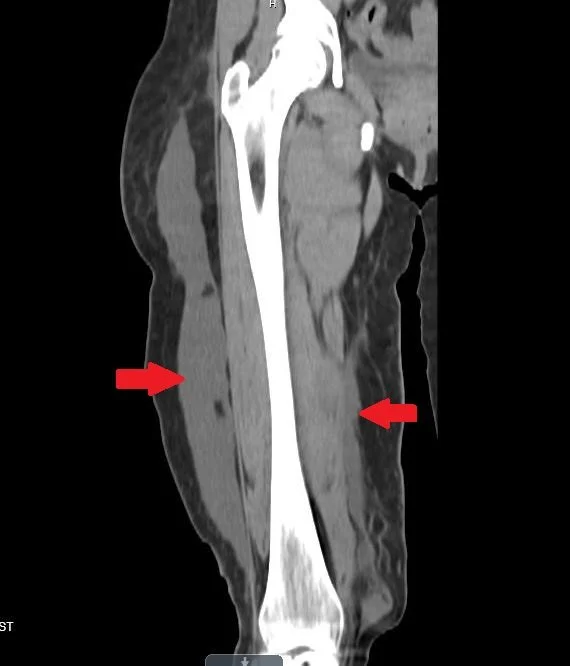
the arrows point to the pathology
Our patient had an internal degloving injury with fluid collecting superficial to the iliotibial band laterally and medially along the superificial fascia of the medial thigh. This is known as a Morel-Lavallee lesion. It was named for a French surgeon Maurice Morel-Lavallee in 1863.

Dr. Morel-Lavelle never became department chair
The lesion is caused by disruption of capillaries resulting in an effusion containing hemolynph and necrotic fat. There is a chronic inflammatory reaction which can lead to the formation of a capsulated lesion which can continue to grow with time. Missing this lesion can result in skin necrosis, pain and infection.
Most often the lesions are in the thigh however trunk, prepatellar and scapular regions have been reported. The lesion can occur with or without a fracture with a fracture of the greater trochanter accounting for more than sixty percent of cases that occur with fractures. While most Morel-Lavellee lesions are associated with high velocity impacts, a similar condition can occur following surgery of the abdomen, and when performing liposuction.
MRI is the modality of choice in discovering this lesion but as in our patient a fluid wave can be seen on physical exam and the collection is often visible on CT.

MRI is the best imaging technique
The differential diagnosis of a mass on the thigh would include: Morel –Lavellee, a hematoma, myositis ossificans or a fat fracture. Myositis ossificans involves the muscle belly and tends to shrink with time while the Morel-Lavellee will grow. A fat fracture most often occurs in the lateral thigh when a blunt force causes the trochanteric fat pad to rupture. The fat fracture is differentiated on US because of hyperechoic material in the fluid collection. US is helpful in differentiating Morel-Lavelle from subcutaneous fat fracture.

fat fracture on US.
Acutely, drainage is recommended to prevent infection. A large fluid collection was noted on US in the ED and the pt was taken to the OR . Surgery was performed with debridement of fluid and necrotic tissue. She recovered without complication.
The time course here and the history that the lesion was growing made a hematoma less likely.

note the clear fluid collection in our patient as opposed to the fat fracture above.
Acutely, drainage is recommended to prevent infection. A large fluid collection was noted on US in the ED and the pt was taken to the OR . Surgery was performed with debridement of fluid and necrotic tissue. She recovered without complication.
Nair A, Nazar P, Sekhar R, Ramachandran P, Moorthy S. Morel-Lavallee lesion: a closed degloving injury that requires real attention. Indian J RadialImaging 2014 Jul-Sep;24(3):288-290.
Mellado J, Perez del Palomar L, Diz L, et al. Long standing Morel-Lavallee lisions of the trochanteric resion and proximal thigh: MRI features in five patients AJR Am J Roentgenol. 2004;182:1289-94.
Diviti S, Gupta N, Hooda K, et al. Morel-Lavallee Lesions-Review of Patophysiology, clinical findings , imaging findings and management J Clin Diagn Res 2017 Apri;11(4): TE01-TE04