A 33 y.o. with a history of depression is found on the basement floor wearing a swim suit and in a pool of urine. Pictured are her urine and vomitus.


She is somnolent; what could she have taken?
Our patient had nephrogenic diabetes insipidus from Lithium. She had texted her mother and told her she had taken 160 pills. Her mother found her in the basement in a pool of urine with empty bottles of Lithium( which she had been prescribed a year earlier) and clonazepam. The reason she was in a pool of urine is that Li causes nephrogenic diabetes insipidus. Her urine was very dilute with a specific gravity of 1.004. In the ED she was rousable to painful stimuli and began to vomit so was intubated for airway protection. She continued to make large volumes of dilute urine after her admission to the ICU.
The name insipidus comes from the old practice of tasting urine to determine the cause of illness. Unlike diabetes mellitus which results in sweet urine, diabetes insipidus creates watery flavorless urine. (tasting urine is no longer recommended). The word diabetes comes from the Greek diabainein ”to pass through” and refers to the excessive amounts of urine in both conditions. In diabetes insipidus more than 2.5 L of urine is produced per day. Li is the most common drug implicated in nephrogenic DI with50% ofpeople on Li chronically developing dilute urines. It is more common in chronic overdose but has been reported with acute overdose.
Nephrogenic DI is caused by conditions affecting aquaporin(porous to water) channels in the tubules which allow water resorption. Aquaporin 2 (AQP2) in the kidney is usually dormant in the intravesicular membrane. When it is needed, vasopression ( antidiuretic hormone) cases the vesicles containing aquaporin to fuse to the membrane and release aquaporin which happens in water retaining states like pregnancy and chf. Li, however, decreases the expression of the AQP2 gene preventing the absorption of water.
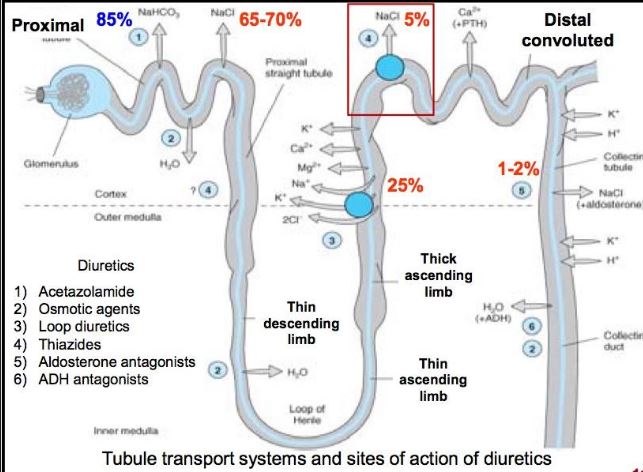
Persons with nephrogenicDI need to consume amounts of fluid equal to the amount excreted but they excrete more water than sodium so serum osmolarity increases which stimulates thirst. Thiazide diuretics are often given to allow increased excretion of sodium, decreasing serum osmolarity and therefore decreasing thirst. This breaks the polydipsia-polyuria cycle. In the case of our patient she was producing 300 cc of urine per hour for several days and these fluids were replaced.
Our patient remained somnolent/intubated because of the clonazepam overdose and although her initial nasal swab was negative for staph, she developed MSSA pneumonia and remained intubated for 8 days. She was extubated on the 8th day and is now alert and oriented agreeing to psychiatric admission.
Clinical pearls: serum lithium levels do not correlate well with clinical findings. Our patient’s Li level rose only to 1.5and yet she had profound polyuria. If sodium rises desmopressin can be given to correct the electrolyte abnormalities. Dialysis is helpful with neurologic toxicity which usually occurs with a Li level of 3 or greater.
Wildin R. What is nephrogenic diabetes insipidus? 2006. The diabetes Insipidus Foundation http://www.diabetes insipidus.org/4-types-nephrogenic-di.htm
Erden A, Karagoz H, et al. Lithium intoxication and nephrogenic diabetes insipidus: a case report and review of literature. Int J Gen med 2013;6:535-539.
Alexander MP, Farag YMK, et al. Lithium toxicity: a double-edged sword. Kidney Int. 2008;73:233-7.

