A 79 y.o. woman is a restrained passenger in a high speed MVC. + LOC . her only complaint is that she is confused.
What do you see on the CXR that might explain her confusion?

Our patient had a stroke most likely caused by embolic phenomenon after an aortic injury. This is not the usual transection since it also involved the subclavian artery with non occlusive thrombus in the proximal vessel. Strokes are more commonly associated with aortic dissection
than transection and have even been reported after being struck in the chest with the recoil after firing a rifle.

The aortic injury is seen in this image with a mediastinal hematoma surrounding.
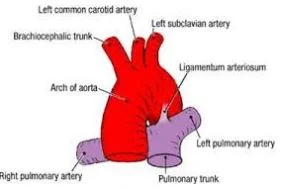
Acute traumatic rupture of the aorta accounts for 18% of all deaths in auto accidents. The most common site of rupture is the proximal descending aorta near where the subclavian branches off. This is where the remnants of the ductus arteriosus are located; the structure that shunts fetal blood from the pulmonary artery to the aorta . Those who do not die immediately(80%) can have an incomplete tear and a false aneurysm. In our patient there was an injury to the aorta and blood dissected both into the mediastinum causing the widened mediastinum on xray and into the pericardium. Probably because of her strokes, the patient did not report chest pain or back pain until later in her course.
Other injuries includedR rib fractures 3-7, a C2 tear drop fracture, and three punctate foci of diffusion restriction on MRI (one in either occipital lobes and one in the R hippocampus) compatible with embolic strokes.

C2 fracture
Our patient had a TEVAR ( thoracic endovascular aortic repair) stent placed and a bypass of L carotid to the L subclavian. A nurse noted that the bp in the R arm was 155/52 and in the L was 70/52 post op. This was due to the vascular procedure and expected; so BP in a patient like this should be taken only in the R arm. She is currently intermittently alert.
Khoynezhad A, Donayre C, Bui H. et al. Risk ofneurodefecit after thorcic aortic endografting. Annals of Thoracic Surgery, 2007. Vol 83(2).
Lobay K, Macgougan C. Traumatic ooronary dissection: a case report and literature reviews. J Em Med 2012 43 e239-43.
Phillips BJ. Traumatic rupture of the thoracic aorta; an endoluminal approach. 2001. Internet Journal of Thoracic and cardiovascular surgery 4(1) 2001do1: 10.5580/2563.
McKnight J, Meyer J, Neville J. Non penetrating traumatic rupture of the thoracic aorta. 1964. Ann Surg 160(6); 1069-1072.
Rao M, Panduranga P, Al-Mukhaini M et al. Ischmic stroke secondary to aortic dissection following rifle butt recoil chest injury. Oman Med J. 2011 26(8) 438-440.