An abnormal CXR
A 38 y.o. female was found unresponsive at the scene of an accident. She was a restrained driver in a car hit head on reportedly by a car going 20 mph. Her car was hit on the passengers side and her airbag deployed. She was unconscious on EMS arrival but awake on arrival to the ED and screaming. GCS was 14. She complained of pain in her back and shortness of breath.
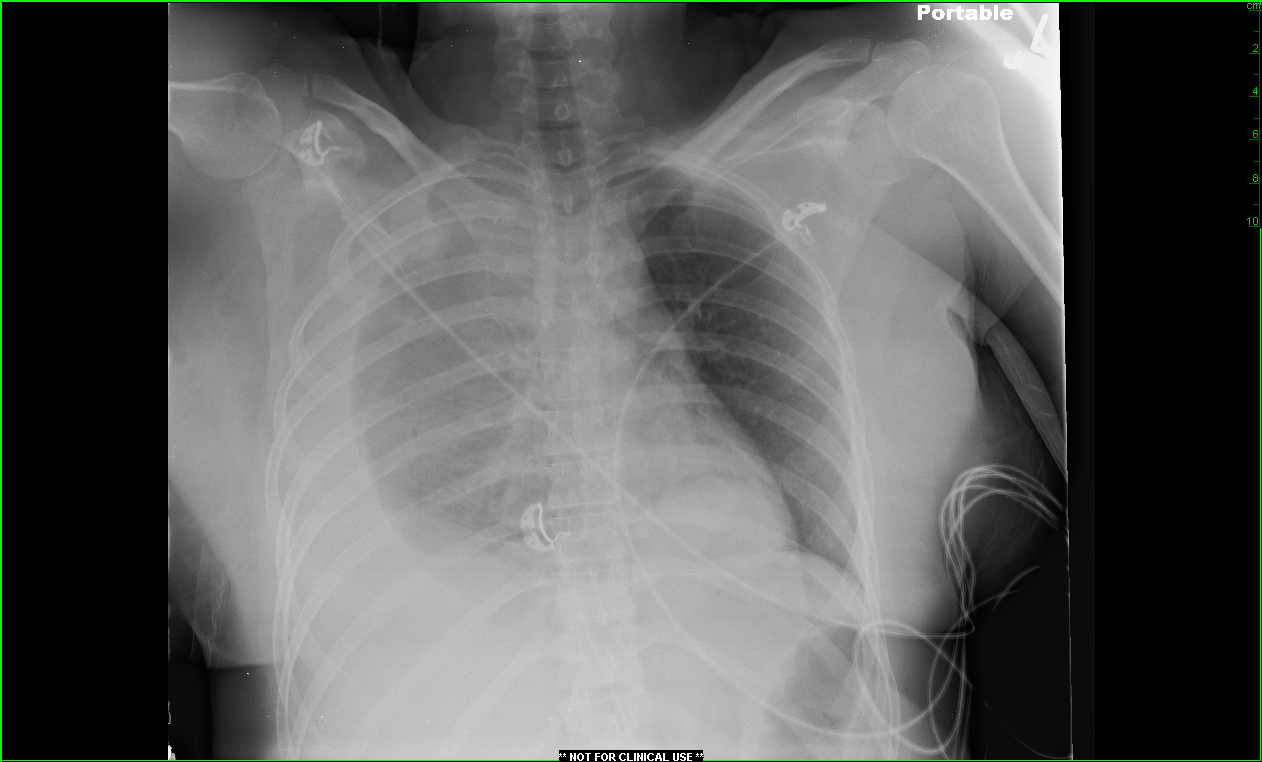
What do you see on the CXR? What would you do next? Scroll down for the Case Conclusion.
Diagnosis: diaphragmatic rupture.
Case Conclusion: In addition to the hemothorax on the right side of the chest (for which a chest tube was placed), it was noted that the patient had a circular opacity in the left chest behind the heart. A CT showed that this opacity represented herniation of the stomach above the diaphragm. The patient went to the OR, where they discovered a 3-4 cm rent in the diaphragm just to the left of the midline above the aortic hiatus and not involving the esophageal hiatus and the diaphragm. About 20% of the stomach was found herniating in through this recent diaphragmatic defect into the chest. The stomach, however, appeared healthy. There was no other injury to her small bowel, her stomach, her liver, spleen, and there was no evidence of retroperitoneal hematomas or pelvic hematomas.
Learning Points: The diagnosis of diaphragmatic rupture following trauma was first made in 1579 by Ambroise Pare, a French barber-surgeon. He found a delayed rupture in an army officer who had been shot 8 months before.

Diaphragmatic injuries appear in 1 to 7% of patients with blunt trauma and 10% of patients with penetrating wounds. Clinically, left sided lesions predominate with right sided injuries occurring only one half as often. This may be because of a cushioning effect of the liver.
The mechanism of diaphragmatic rupture is uncertain although Kearney postulatedthat a direct anterior blow to the abdomen may increase intrabdominal pressure and exceed the bursting pressure of the diaphragm. He also proposed that a lateral blow can cause a sheer forcewhich can result in detachment of the diaphragm from its insertion on the chest wall.
Penetrating trauma such asstabandgunshotwounds result in injury to the diaphragm more often than blunt trauma. A gunshot woundanywhere within the within the chest or abdomen puts the patient ata riskfor penetrating diaphragmatic traumabecause of the potentially prolonged length of travel of the projectile within the body. Stab wounds between the nipple and the umbilicus are the ones most likely to cause significant damage. In the case of penetrating trauma it is possible for a diaphragmatic injury to occur without the immediate herniation of bowel contents into the chest, although they may herniate over time resulting in a delayed presentation. Therefore, the diagnosis of diaphragmatic rupture requires a high index of suspicion. Although CT scanning has improved the chances that the diagnosis will be made before surgery, only 31-43% diaphragm ruptures are diagnosed prior to surgery. Although an injury to the diaphragm was suspected in this case; it was not diagnosed on CT scan.

One other thing demonstrated by this case is the concept of “satisfaction of search”. When looking at the CXR, it is easy to see the hemopneumothorax on the right and ignore the left diaphragm because you stop searching. Agood search strategy on the CXR involves looking at the “I”; the top horizontal of the “I” being the clavicles, the vertical part of the “I” being the trachea and spine and the bottom horizontal part of the “I” being the diaphragms. Make sure to evaluate the chest X-ray completely, especially in the face of obvious injury.
Case Conclusion by Dr. Roseanne Naunheim
References:
1. Kearney PA, Rouhana SW, Burney RE. Blunt rupture of the diaphragm: mechanism, diagnosis , and treatment. Ann of Emerg Med 1989;18: 1326-30.
2. Boulanger BR, Mirvis SE, Rodriguez A. Magnetic resonance imaging in diaphragmatic rupture: case reports. J Trauma 1992;32:89-93
3. Sarna S, Kivioja A. Blunt rupture of the diaphragm. Ann Chir Gynaecol 1995;84:261-5.
4. ScharffJR. Naunheim KS. Traumatic Diaphragmatic Injuries. Chest Surg Clin NA 2007; 17:81-5.
5. Weyant MJ. Fullerton DA (2008) “Blunt thoracic trauma”. Seminars in Thoracic and Cardiovascular Surgery 20 (1): 26-30.