Hippocratic Medicine No. 4: Victims of Our Own Success?

Clinical Scenario:
Working a emergency department shift on a typical busy day, you see the next patient slotted is a 36-year-old female coming in with shortness of breath and fatigue. She also has a history of anemia, anxiety, and panic disorder.
About one month prior, she presented to another emergency department (ED) complaining of chest pain for the last several weeks along with other vague complaints. Her heart rate of 101 prevented application of the PERC rule and made her moderate risk by Well’s criteria. A d-dimer was sent and was elevated, so she underwent a computed tomography pulmonary angiography (CTPA) scan looking for pulmonary embolism (PE). This demonstrated non-occlusive pulmonary emboli present in branches of the left upper lobe, right middle lobe, and left lower lobe pulmonary arteries. She was admitted to the hospital and started on rivaroxaban.
About 2 weeks prior to today’s visit, she had presented with continued chest pain and shortness of breath. She underwent another CTPA demonstrating no pulmonary emboli. Her hemoglobin was checked on this visit and found to be 11 g/dl. She was discharged and continued taking her rivaroxaban.
During to today’s visit, in addition to her shortness of breath and fatigue, she is also complaining of vaginal bleeding. It is around the normal time for menses, however it has been going on longer and heavier than usual. Her hemoglobin is checked and is found to be 5.6 g/dl. She is given two units of packed red blood cells and admitted to the hospital.
You can’t help but wonder, was there truly a PE in the first place? Did it require treatment? Did we cause this patient harm by putting her on anticoagulation?
Literature review:
The diagnosis of PE has evolved significantly over the past few decades from a disease only suspected and confirmed on autopsy to small subsegmental pulmonary embolisms (SSPE) found on multi-detector CTPA. Despite the increased diagnosis of PE due to CTPA, there has not been a significant change in associated mortality nor an increase in diagnosis of larger, central pulmonary emboli [2]. What has changed is the increased diagnosis of smaller sub-segmental pulmonary embolism (SSPE) due likely to both the sensitivity of the technology and increased physician vigilance for finding the disease [1].
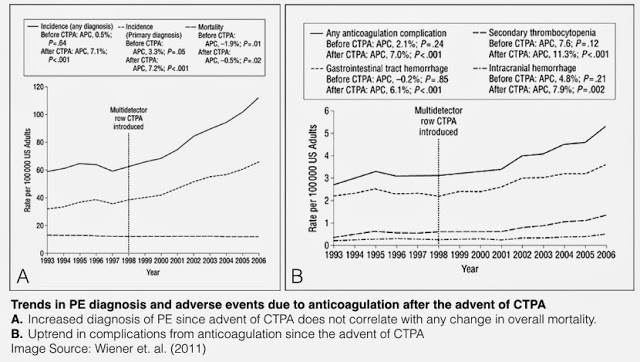
Not long ago, pulmonary embolism was felt to be under-diagnosed, only found after the patient had died from the condition. With the widespread availability and ease of CTPA, there is increasingly concern for overuse of CTPA, perhaps with associated over-diagnosis and over-treatment. Wiener et al studied the incidence, mortality, and treatment complications of PE in the 5 years preceding the introduction of CTPA and the years that followed [2]. With the introduction of CTPA, he found that the diagnosis of PE almost doubled (62.1 to 112.3 per 100,000) and complications from anticoagulation increased (3.1 to 5.3 per 100,000), while the mortality from PE stayed about the same (12.3 to 11.9). While the increase in diagnosis is probably due to increased awareness of PE as well as availability of testing, some of the increase may also be due to the detection of smaller SSPE on multi-detector CTPA that may not be clinically relevant [3].
As a large proportion of the additional PEs detected (above the prior baseline) are SSPEs [3], and in light of the increase in bleeding complications from anticoagulation, this raises the question as to whether the risks of treatment outweigh the risks of going untreated. A study in CHEST demonstrated that hemodynamically stable patients with segmental or sub-segmental PE had low risk of adverse outcome, although in this study population treatment was at the discretion of the treating physician [6]. In a review paper by Ikesaka and Carrier, they found that patients with suspected PE with a non-diagnostic ventilation-perfusion scan and negative compression ultrasonography of the lower extremities could be safely managed without the use of anticoagulation with a recurrent risk of embolism similar to those without PE on CTPA [1]. In addition, 17% of patients with a low probability ventilation/perfusion (V/Q) scan had an isolated SSPE on CTPA.
Despite many physicians treating it otherwise, CTPA is not a gold standard for PE diagnosis. Up to 11% of CTPA studies read initially positive for SSPE are read as negative when reviewed by experienced thoracic radiologist. These 'false positives' may be caused by indeterminate intra-luminal filling defects that may be caused by patient motion artifact or other imaging artifact [4,7].
In addition to the potential harm in placing someone unnecessarily on anticoagulation, testing for PE can also cause harm. The radiation from the scan can cause promote cancer later in the patient’s life while the contrast can induce nephropathy. In a conservative estimate by Newman and Schriger, they found that in testing for PE, physicians can prevent 6 deaths from PE and 24 major, nonfatal PE events per 10,000 individuals [8]. At the same time, testing also can cause 36 deaths and 37 nonfatal major medical harms per 10,000 from bleeding complications, development of cancer, and contrast-induced nephropathy. This estimates seems to imply that physicians can cause more harm than benefit in testing for PE if the diagnostic test is not applied judiciously to patients.
With the introduction of CTPA, there has been a substantial increase in the diagnosis of PE, especially SSPE, without much apparent clinical benefit with treatment. Are we over-diagnosing more patients and putting them on treatments with potential harm? Do we need to scan or even treat these patients? In this presented case, did this patient truly have a PE given that a repeat scan 2 weeks later was read as completely negative? Did this patient bleed down to a hemoglobin of 5.6 g/dl because of the treatment she was on?
Take home points:
- Pulmonary embolism may be over-diagnosed and over-treated
- Be aware of the false positive rate with CTPA and consider this when deciding whom to test
- There’s evidence to suggest not all PE’s are the same, but there is insufficient ED-based data to determine who should receive anticoagulation
-Realize that you can cause harm putting a patient on anticoagulation when it is not necessarily needed
Submitted by Steven Hung, PGY-2 (@docHungER)
Edited by Alicia Oberle, PGY-3
Faculty Reviewed by Ryan Schneider, Richard Griffey, and Chris Carpenter (@SAEMEBM)
Image by Maia Dorsett (@maiadorsett)
Want to read more? Click here to read the WashU Journal Club on reducing PE protocol CT ordering rates in the ED.
References:
1. Ikesaka F, Carrier M. Clinical significance and management of sub-segmental pulmonary embolism. J Thromb Thrombolysis. 2015 Apr;39(3):311-4.
2. Wiener RS, Schwartz LM, Woloshin S. Time trends in pulmonary embolism in the United States: evidence of overdiagnosis. Arch Intern Med. 2011;171(9):831-837
3. Carrier M, Righini M, Wells PS, Perrier A, Anderson DR, Rodger MA, Pleasance S, Le Gal G. Subsegmental pulmonary embolism diagnosed by computed tomography: incidence and clinical implications. A systematic review and meta-analysis of the management outcome studies. J Thromb Haemost. 2010 Aug;8(8):1716-22.
4. Jones SE, Wittram C. The indeterminate CT pulmonary angiogram: imaging characteristics and patient clinical outcome. Radiology. 2005 Oct;237(1):329-37.
5. Prasad V, Rho J, Cifu A. The diagnosis and treatment of pulmonary embolism: a metaphor for medicine in the evidence-based medicine era. Arch Intern Med. 2012 Jun 25;172(12):955-8.
6. Vedovati MC, Becattini C, Agnelli G, Kamphuisen PW, Masotti L, Pruszczyk P, Casazza F, Salvi A, Grifoni S, Carugati A, Konstantinides S, Schreuder M, Golebiowski M, Duranti M. Multidetector CT scan for acute pulmonary embolism: embolic burden and clinical outcome. Chest. 2012 Dec; 142(6):1417-24.
7. Wittram C, Maher MM, Yoo AJ, Kalra MK, Shepard JA, McLoud TC. CT angiography of pulmonary embolism: diagnostic criteria and causes of misdiagnosis. Radiographics. 2004 Sep-Oct;24(5):1219-38.
8.Newman DH, Schriger DL. Rethinking testing for pulmonary embolism: less is more. Ann Emerg Med. 2011 Jun;57(6):622-627.e3.
The Hippocratic Medicine series is modeled after the Do No Harm project pioneered at the University of Colorado. The aim of this series is to raise awareness about the avoidance of avoidable care i.e. for how medical overuse has the potential to do patient harm. Because every test or intervention we do has the potential for not just benefit but also harm, we should seek that our patients do better because of the care we provide instead of despite it. The WUSM Hippocratic Medicine Series is supported by a grant provided by the Foundation for Barnes Jewish Hospital.