EKG Challenge No. 16 Case Conclusion
A 76 year-old male with a history of severe ischemic cardiomyopathy with an ejection fraction of 15%, atrial fibrillation on coumadin, coronary artery disease, and chronic kidney disease is brought in by paramedics from a skilled nursing facility with confusion, somnolence, and vomiting. Per EMS report, the patient has been vomiting for two or three days.
On arrival, the patient’s blood pressure is 128/78 with a heart rate of 130 and oxygen saturation of 99% on room air. On exam, he is oriented to self only. He is slightly agitated but following commands. He has some mild garbled speech and is moving all extremities well. He denies chest pain, dyspnea, or abdominal pain. His extremities are well perfused with intact peripheral pulses and preserved capillary refill. A full set of labs are drawn and pending. A head CT is performed and shows an intracranial hemorrhage and small subarachnoid hemorrhage.
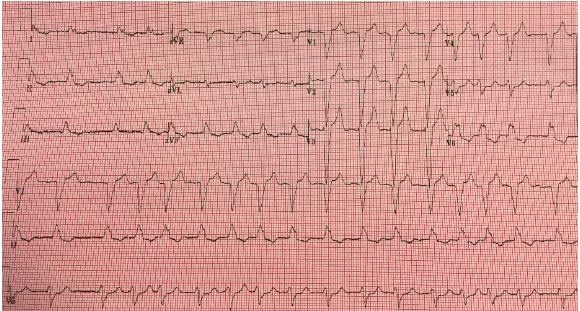
A standard 12-lead EKG is performed:

This EKG shows an irregular wide-complex tachycardia. Given the patient’s history and these findings, there are several pertinent diagnostic considerations:
Polymorphic ventricular tachycardia (VTach): The patient has multiple risk factors for acute coronary syndrome and known structural heart damage. He is thus at high risk of lethal arrhythmia such as VTach.
Atrial fibrillation with aberrancy: The patient has known atrial fibrillation and ischemic cardiomyopathy. He could easily have myocardial scarring that could create a left bundle branch block. His tachycardia could be due to rapid ventricular response, or it could be compensatory due to volume depletion.
Atrial fibrillation with preexcitation: Along similar lines, the patient could easily have scarring that could create an accessory conduction pathway.
Hyperkalemia: The patient has known chronic kidney disease and is likely dehydrated due to his vomiting. The bizarre QRS morphology and high T waves could suggest hyperkalemia.
Before considering treatment options, we need to decide if the patient is stable or unstable. Although the patient is markedly tachycardic, his blood pressure is in the normal range. His mental status is altered, but this is easily explained by his intracranial hemorrhage, and his physical exam suggests that his perfusion is not acutely compromised. We can thus treat this patient as stable, and we do not need to perform immediate electrical cardioversion (although it would be prudent to put the defibrillator pads on, just in case the patient decompensates). Remember: in stable patients with a complex differential, “don’t just do something, stand there” and take your time to consider your options.
We have several options for treatment: adenosine, other AV nodal blockers such as beta blockers or calcium channel blockers, and antiarrhythmics such as amiodarone or procainamide. However, given the patient’s complex medical history and the broad differential we outlined above, all of these treatments are problematic in the acute phase.
Adenosine can be considered in regular wide-complex tachycardias (WCTs), as it can slow down the heart rate and help unmask the underlying rhythm or accessory pathways. However, in irregular WCTs, blocking the AV-node could increase conduction through an accessory pathway, leading to treatment-resistant refractory tachydysrhythmias. Calcium channel blockers and beta-blockers also have the potential to increase conduction through an accessory pathway. Additionally, they have a negative inotropic effect, which could exacerbate this patient’s already severe heart failure and precipitate cardiopulmonary deterioration.
Antiarrhythmics such as procainamide or amiodarone might be a reasonable choice. The American Heart Association recommends amiodarone for stable wide-complex tachycardias, but it can be dangerous in the setting of rapid atrial fibrillation with preexcitation, as it can cause AV nodal blockade. Procainamide has been shown to be effective in all types of wide complex tachycardias, and is the drug of choice in rapid atrial fibrillation with preexcitation. Recent studies have suggested that it might be equivalent or even superior to amiodarone for in VTach. However, it also has negative inotropic effects and is thus dangerous in patients with heart failure. Lidocaine has variable evidence in regards to efficacy of cardioversion, AV-nodal blockade, and inotropic effects, but may be as effective as amiodarone for VTach. Furthermore, administration of any of these sodium channel blocking agents could be dangerous if the patient truly is hyperkalemic, as severe hyperkalemia can potentiate sodium channel blockade and induce asystole.
There is no ideal answer for this patient given his co-morbidities and the severity of his heart failure. The safest choice is probably elective cardioversion. However, cardioversion is frequently unsuccessful in patients with abnormal hear architecture and chronic arrhythmias. If an antiarrhythmic agent must be given, amiodarone is probably the safest choice. Given that the patient is stable, we can likely attend to his other urgent medical problems and await some lab results (specifically, a BMP or whole blood potassium).
Case Conclusion:
The patient’s BMP shows a serum potassium of 7.2 and a creatinine of 4.2, suggesting acute renal failure with severe hyperkalemia.
Hyperkalemia generally produces a spectrum of ECG findings that classically progress as serum potassium rises. Peaked T-waves (tall and narrow) are often the initial abnormality seen on ECG. P-wave flattening and PR lengthening generally follow; in this case, the patient’s atrial fibrillation precludes evaluation of his (absent) P waves. As the serum potassium level continues to rise, the QRS interval begins to widen. Bizarre QRS morphology develops and can progress into a sine wave pattern in advanced hyperkalemia. Ultimately, this can lead to VFib or asystole.
Classic teaching notwithstanding, severity of hyperkalemia is very difficult to evaluate based on EKG alone. Not for nothing is hyperkalemia called “the syphilis of the EKG.” We can, however, identify both high T waves and bizarre widended QRS complexes on this patient’s EKG.
The patient was treated with calcium, insulin, and dextrose for acute stabilization. Repeat EKGs (shown below) demonstrated interval normalization of electrical morphology with resolution of acute hyperkalemia. Ultimately, Renal was consulted for acute dialysis, and the patient was admitted to the Neurosurgical ICU for management of his intracranial hemorrhage.
Repeat EKG #1, after treatment for hyperkalemia

Repeat EKG #2, after treatment for hyperkalemia
Take-Home Points:
Generally, treat wide-complex tachycardias as ventricular tachycardia until proven otherwise, but be suspicious of hyperkalemia in any patient with a wide-complex tachycardia and renal insufficiency.
In any unstable patient with a tachydysrhythmia, proceed to emergent cardioversion. In stable patients, don’t be afraid to take some time to consider alternative diagnose and await critical lab results.
References:
1) Emerg Med Practice. 2008;10(4):1-28
3) N Engl J Med. 2016;374(18):1711-22
4) Ann Emerg Med 2000;36:615-27
Case submitted by Mike Willman PGY-3
Everyday EBM Editor Kevin Baumgartner PGY-2
Faculty reviewed by Chandra Aubin MD