EKG Challenge No. 14 Case Conclusion: The EKG Sign Formerly Known as Prince?
On a Sunday afternoon, an elderly gentleman is brought into the
emergency department by his wife complaining of chest pain that began
one hour ago. He is diaphoretic and appears very uncomfortable. An EKG is
obtained. The patient has no prior EKGs available.
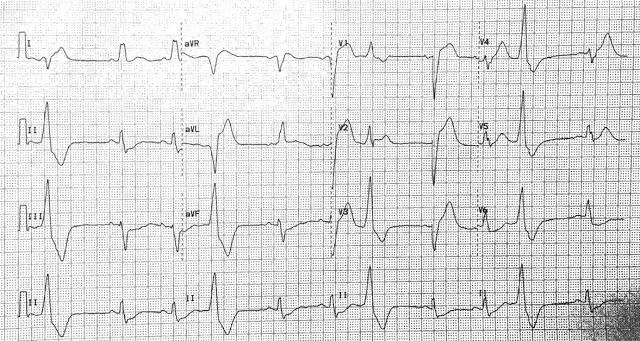
When you first look at the EKG, you note that there appears to be an abundance of PVCs... ventricular trigeminy actually. Given the patient's clinical appearance, you suspect an acute MI.... now to just sort out the EKG to support your clinical gestalt.
Given the prevalence of ventricular ectopy, you begin your analysis by identifying sinus beats [although you can use PVCs as well - see these posts (1) and (2) on Dr. Smith's ECG blog]:
If you take one sinus tracing for each lead:
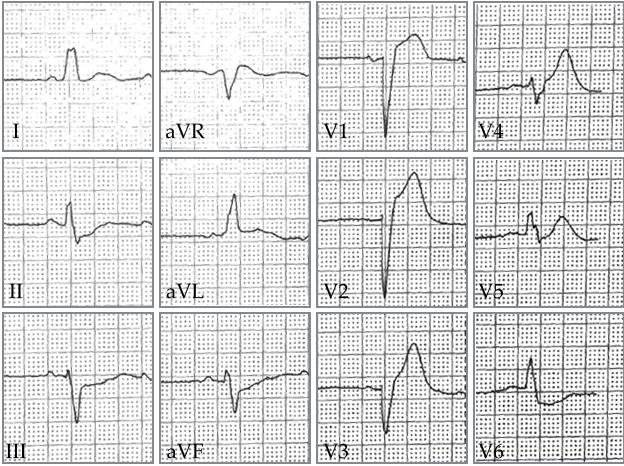
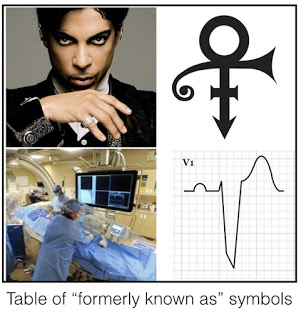
Secondly, you observe that the tracing follows left bundle branch block (LBBB) morphology. New LBBB may be considered the criteria "formerly known as" an indication for cath lab activation.
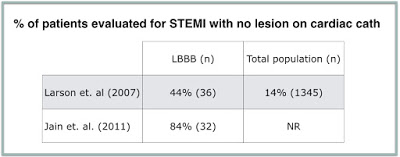
 The 2004 ACC/AHA STEMI guidelines included new LBBB as a indication for Cath lab activation in patients presenting with symptoms suspicious for acute MI. This was changed in the 2013, largely due to data suggesting that this was responsible for a large number of "false positive" cath lab activations [1]. Two separate studies involving patients with LBBB evaluated for suspected STEMI found an overall low prevalence of coronary lesions amenable to PCI [2,3].
The 2004 ACC/AHA STEMI guidelines included new LBBB as a indication for Cath lab activation in patients presenting with symptoms suspicious for acute MI. This was changed in the 2013, largely due to data suggesting that this was responsible for a large number of "false positive" cath lab activations [1]. Two separate studies involving patients with LBBB evaluated for suspected STEMI found an overall low prevalence of coronary lesions amenable to PCI [2,3].
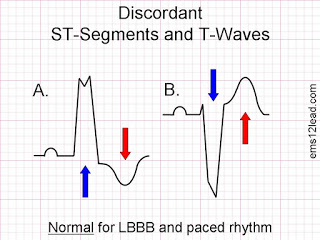
In "normal" LBBB, repolarization is characterized by ST segment and T wave deviation away from the major direction of the terminal QRS waveform - also known as "appropriate discordance" [1]. Hence, in leads where the QRS is positive, the ST segment (and often the T wave) are deflected in the opposite direction and vice versa:
Appropriate discordance makes it more difficult, but not impossible, to assess for acute myocardial infarction with underlying LBBB. In 1996, Sgarbossa and colleagues retrospectively derived and independently validated a clinical prediction rule for EKG diagnosis of acute myocardial infarction in the context of LBBB using positive biomarkers as a gold standard [4]. These three criteria are illustrated in the figure below:
There are few important things to note about the Sgarbossa criteria. First, Sgarbossa criteria only need to be met in a single lead. Second, the three criteria are not equal in their sensitivity or specificity with respect to predict myocardial infarction and thus are awarded different points within the model. In the initial study, concordant ST elevation was found to have a sensitivity of 73% (95% CI 64-80) and specificity of 95% (95% CI 86-96), while concordant ST segment depression had a sensitivity of only 25% (95% CI 18-34) and specficity of 96% (95% CI 91-99). The third criteria, discordant ST segment elevation > 5 mm, has a sensitivity of 31% (95% CI 23-39) and specificity of 92% (95% CI 85-96). Thus, the Sgarbossa criteria were specific, but not necessarily sensitive, for acute myocardial infarction as diagnosed by positive biomarkers.
A meta-analysis of subsequent studies evaluating the Sgarbossa criteria was published in 2008 [5]. Based on calculated sensitivities and specificities (see below), this study recommended at the Sgarbossa score of > 3 (i.e. only concordant ST elevation anywhere or concordant ST depression in V1, V2 or V3) physicians should treat for acute myocardial infarction. A Sgarbossa score of 2 (i.e. meeting the discordant criteria alone) was deemed "inadequate to diagnose myocardial infarction."
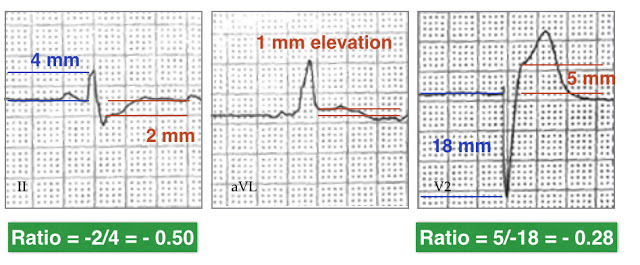
Smith et. al. (2012) addressed the low sensitivity of the initial Sgarbossa criteria by postulating that changing the third component (excessive discordance) to a proportional rule instead of a 5 mm absolute cutoff would increase both the sensitivity and specificity of the criteria. They defined "Abnormal, excessive discordance" as a ST/S ratio of < -0.25.
The authors proposed a "modified" unweighted Sgarbossa criteria:
1. Concordant ST elevation > 1 mm in any lead
2. ST segment depression > 1 mm in V1, V2 or V3
3. ST/S ratio < -0.25 in any lead with > 1 mm of ST segment elevation or depression
The EKG was considered positive for ischemia if any of the above criteria were met.
Based on a data set using angiographic occlusion or troponin value > 10 ng/mL as their cutoff for "true MI", they calculated a sensitivity of 91% (95% CI 76-98) and specificity 90% (83-95) for the Modified Sgarbossa criteria.
If we apply the Sgarbossa and Modified Sgarbossa criteria to our patient's EKG, the patient meets criteria for acute myocardial infarction.
The patient did go to the cardiac catheterization laboratory and was found to have a 100% occlusion of the mid-LAD:
So what would happen if this patient did not meet Sgarbossa criteria? Remember Sgarbossa criteria are far from sensitive. The modified Sgarbossa criteria significantly improve on this, but has not yet been validated in a distinct set of EKGs. What would you do?
When this patient presented, the cardiologist was at first reticent to take him to the cath lab. Rather than arguing technicalities on a Sunday afternoon, the attending physician, Heather Webb (@webbmd) used what I would say are some of the most important criteria in a patient who looks sick and has severe chest pain, diaphoresis and a presumed new left bundle branch block to demand that the patient go: Clinical Gestalt.
Take Home Points: Left bundle branch block makes the diagnosis of acute myocardial infarction more difficult. The original Sgarbossa criteria developed in 1996 aimed at identifying myocardial infarction in the context of LBBB were specific but poorly sensitive. These were improved with development of the Modified Sgarbossa criteria, which incorporated the concept for proportionality in the evaluation of ST/S discordance. Remember that these rules do not fully account for your pretest probability or clinical gestalt of when a patient is having an MI. If the patient looks like they are having an MI and has a new left bundle branch block, they should probably go to the cath lab regardless. Now for Prince's Song of the Heart...
Submitted by Maia Dorsett, PGY-4 (@maiadorsett)
Faculty Reviewed by Doug Char and Joan Noelker
Interested in reading additional resources (Thanks to@tbouthillet for sharing):
- ECG Medical Training on the Modified Sgarbossa criteria
- Dr. Smith's ECG blog on Modified Sgarbossa criteria with links to additional cases
- ALiEM discussion of Modifed Sgarbossa criteria with management algorithm for new LBBB
References
1. Cai, Q., Mehta, N., Sgarbossa, E. B., Pinski, S. L., Wagner, G. S., Califf, R. M., & Barbagelata, A. (2013). The left bundle-branch block puzzle in the 2013 ST-elevation myocardial infarction guideline: from falsely declaring emergency to denying reperfusion in a high-risk population. Are the Sgarbossa Criteria ready for prime time?. American heart journal, 166(3), 409-413.
2. Larson, D. M., Menssen, K. M., Sharkey, S. W., Duval, S., Schwartz, R. S., Harris, J., ... & Henry, T. D. (2007). “False-positive” cardiac catheterization laboratory activation among patients with suspected ST-segment elevation myocardial infarction. Jama, 298(23), 2754-2760.
3.Jain, S., Ting, H. T., Bell, M., Bjerke, C. M., Lennon, R. J., Gersh, B. J., ... & Prasad, A. (2011). Utility of left bundle branch block as a diagnostic criterion for acute myocardial infarction. The American journal of cardiology, 107(8), 1111-1116.
4. Sgarbossa, E. B., Pinski, S. L., Barbagelata, A., Underwood, D. A., Gates, K. B., Topol, E. J., ... & Wagner, G. S. (1996). Electrocardiographic diagnosis of evolving acute myocardial infarction in the presence of left bundle-branch block. New England Journal of Medicine, 334(8), 481-487.
5. Tabas, J. A., Rodriguez, R. M., Seligman, H. K., & Goldschlager, N. F. (2008). Electrocardiographic criteria for detecting acute myocardial infarction in patients with left bundle branch block: a meta-analysis. Annals of emergency medicine, 52(4), 329-336.
6. Smith, S. W., Dodd, K. W., Henry, T. D., Dvorak, D. M., & Pearce, L. A. (2012). Diagnosis of ST-elevation myocardial infarction in the presence of left bundle branch block with the ST-elevation to S-wave ratio in a modified Sgarbossa rule. Annals of emergency medicine, 60(6), 766-776.
 |
| Sinus beats outlined in blue. Other beats are premature ventricular contractions (PVCs) |
Secondly, you observe that the tracing follows left bundle branch block (LBBB) morphology. New LBBB may be considered the criteria "formerly known as" an indication for cath lab activation.
In "normal" LBBB, repolarization is characterized by ST segment and T wave deviation away from the major direction of the terminal QRS waveform - also known as "appropriate discordance" [1]. Hence, in leads where the QRS is positive, the ST segment (and often the T wave) are deflected in the opposite direction and vice versa:
Appropriate discordance makes it more difficult, but not impossible, to assess for acute myocardial infarction with underlying LBBB. In 1996, Sgarbossa and colleagues retrospectively derived and independently validated a clinical prediction rule for EKG diagnosis of acute myocardial infarction in the context of LBBB using positive biomarkers as a gold standard [4]. These three criteria are illustrated in the figure below:
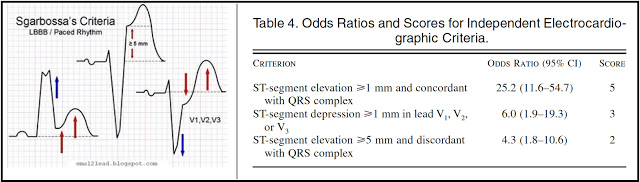 |
| Image source: ecg12lead; Table source: Sgarbossa et. al. (1996) |
There are few important things to note about the Sgarbossa criteria. First, Sgarbossa criteria only need to be met in a single lead. Second, the three criteria are not equal in their sensitivity or specificity with respect to predict myocardial infarction and thus are awarded different points within the model. In the initial study, concordant ST elevation was found to have a sensitivity of 73% (95% CI 64-80) and specificity of 95% (95% CI 86-96), while concordant ST segment depression had a sensitivity of only 25% (95% CI 18-34) and specficity of 96% (95% CI 91-99). The third criteria, discordant ST segment elevation > 5 mm, has a sensitivity of 31% (95% CI 23-39) and specificity of 92% (95% CI 85-96). Thus, the Sgarbossa criteria were specific, but not necessarily sensitive, for acute myocardial infarction as diagnosed by positive biomarkers.
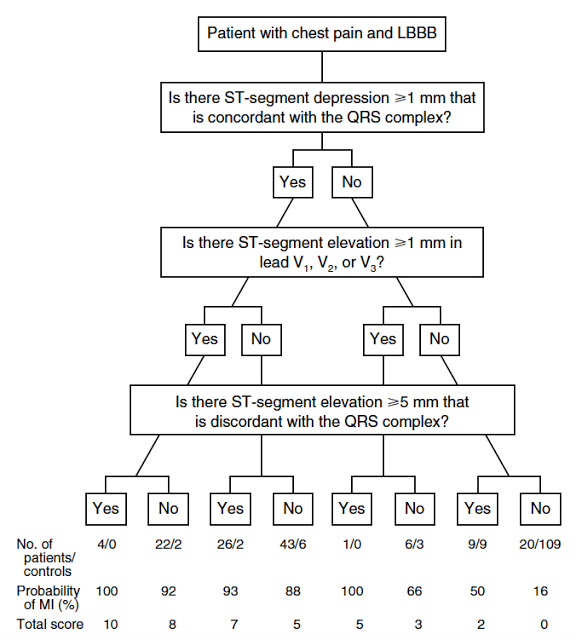 |
| Source: Sgarbossa et. al. (1996) |
A meta-analysis of subsequent studies evaluating the Sgarbossa criteria was published in 2008 [5]. Based on calculated sensitivities and specificities (see below), this study recommended at the Sgarbossa score of > 3 (i.e. only concordant ST elevation anywhere or concordant ST depression in V1, V2 or V3) physicians should treat for acute myocardial infarction. A Sgarbossa score of 2 (i.e. meeting the discordant criteria alone) was deemed "inadequate to diagnose myocardial infarction."
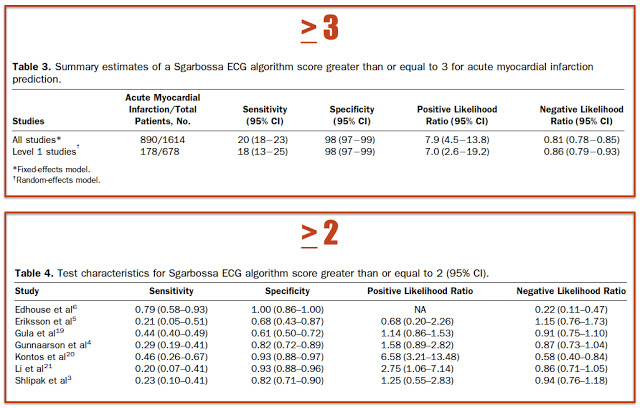 |
| Source: Reference 5 |
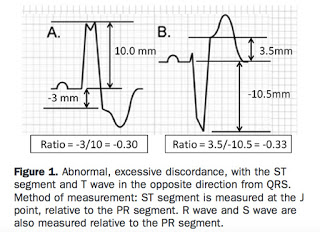 |
| Image Source: Smith et. al. (2012) |
1. Concordant ST elevation > 1 mm in any lead
2. ST segment depression > 1 mm in V1, V2 or V3
3. ST/S ratio < -0.25 in any lead with > 1 mm of ST segment elevation or depression
The EKG was considered positive for ischemia if any of the above criteria were met.
Based on a data set using angiographic occlusion or troponin value > 10 ng/mL as their cutoff for "true MI", they calculated a sensitivity of 91% (95% CI 76-98) and specificity 90% (83-95) for the Modified Sgarbossa criteria.
If we apply the Sgarbossa and Modified Sgarbossa criteria to our patient's EKG, the patient meets criteria for acute myocardial infarction.
The patient did go to the cardiac catheterization laboratory and was found to have a 100% occlusion of the mid-LAD:
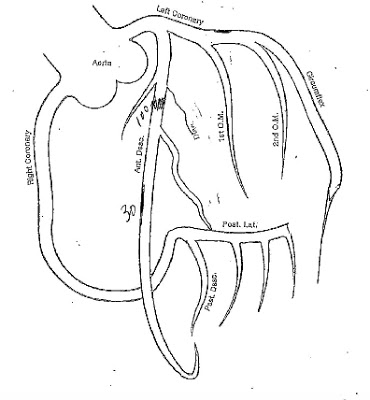 |
| Cath lab diagram demonstrating 100% occlusion of mid-LAD |
When this patient presented, the cardiologist was at first reticent to take him to the cath lab. Rather than arguing technicalities on a Sunday afternoon, the attending physician, Heather Webb (@webbmd) used what I would say are some of the most important criteria in a patient who looks sick and has severe chest pain, diaphoresis and a presumed new left bundle branch block to demand that the patient go: Clinical Gestalt.
Take Home Points: Left bundle branch block makes the diagnosis of acute myocardial infarction more difficult. The original Sgarbossa criteria developed in 1996 aimed at identifying myocardial infarction in the context of LBBB were specific but poorly sensitive. These were improved with development of the Modified Sgarbossa criteria, which incorporated the concept for proportionality in the evaluation of ST/S discordance. Remember that these rules do not fully account for your pretest probability or clinical gestalt of when a patient is having an MI. If the patient looks like they are having an MI and has a new left bundle branch block, they should probably go to the cath lab regardless. Now for Prince's Song of the Heart...
Submitted by Maia Dorsett, PGY-4 (@maiadorsett)
Faculty Reviewed by Doug Char and Joan Noelker
Interested in reading additional resources (Thanks to
- ECG Medical Training on the Modified Sgarbossa criteria
- Dr. Smith's ECG blog on Modified Sgarbossa criteria with links to additional cases
- ALiEM discussion of Modifed Sgarbossa criteria with management algorithm for new LBBB
References
1. Cai, Q., Mehta, N., Sgarbossa, E. B., Pinski, S. L., Wagner, G. S., Califf, R. M., & Barbagelata, A. (2013). The left bundle-branch block puzzle in the 2013 ST-elevation myocardial infarction guideline: from falsely declaring emergency to denying reperfusion in a high-risk population. Are the Sgarbossa Criteria ready for prime time?. American heart journal, 166(3), 409-413.
2. Larson, D. M., Menssen, K. M., Sharkey, S. W., Duval, S., Schwartz, R. S., Harris, J., ... & Henry, T. D. (2007). “False-positive” cardiac catheterization laboratory activation among patients with suspected ST-segment elevation myocardial infarction. Jama, 298(23), 2754-2760.
3.Jain, S., Ting, H. T., Bell, M., Bjerke, C. M., Lennon, R. J., Gersh, B. J., ... & Prasad, A. (2011). Utility of left bundle branch block as a diagnostic criterion for acute myocardial infarction. The American journal of cardiology, 107(8), 1111-1116.
4. Sgarbossa, E. B., Pinski, S. L., Barbagelata, A., Underwood, D. A., Gates, K. B., Topol, E. J., ... & Wagner, G. S. (1996). Electrocardiographic diagnosis of evolving acute myocardial infarction in the presence of left bundle-branch block. New England Journal of Medicine, 334(8), 481-487.
5. Tabas, J. A., Rodriguez, R. M., Seligman, H. K., & Goldschlager, N. F. (2008). Electrocardiographic criteria for detecting acute myocardial infarction in patients with left bundle branch block: a meta-analysis. Annals of emergency medicine, 52(4), 329-336.
6. Smith, S. W., Dodd, K. W., Henry, T. D., Dvorak, D. M., & Pearce, L. A. (2012). Diagnosis of ST-elevation myocardial infarction in the presence of left bundle branch block with the ST-elevation to S-wave ratio in a modified Sgarbossa rule. Annals of emergency medicine, 60(6), 766-776.